This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
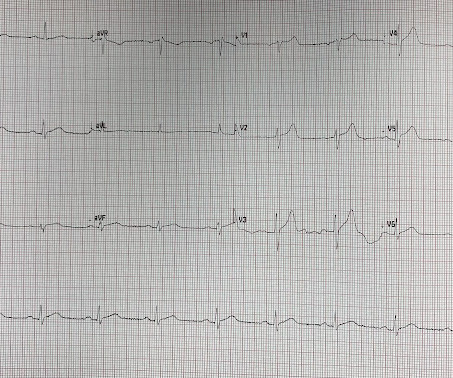
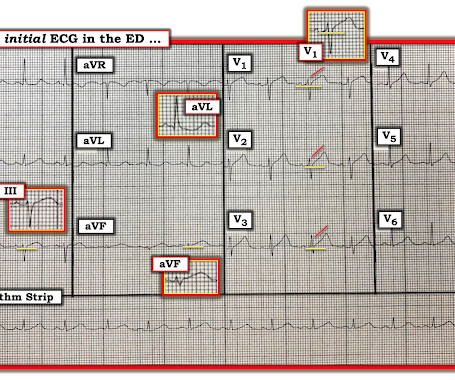
== P lease N OTE : After today — No new ECG Blog posts for 2- to -3 weeks. — I will also not be prompt in replying to emails. == All material on this ECG Blog site remains open! IF you scroll down a little on the right-hand column of this blog — You'll see a lot of icons. Figure-1: The initial ECG in today's case.
Due to the chest pain radiating into the patient's back, the ER physician ordered CTA chest to rule out aortic dissection. But seeing them all together is more suggestive that pericarditis could be possible. While awaiting the results of the CT, the physician called cardiology.
Blog Global Differences in Managing Patients with Aortic Valve Disease KCummings Thu, 10/24/2024 - 09:42 Adult Cardiac All Members It is time to reconsider the management of Aortic valve Disease (AVD) across the world. However, a vast need remains for more affordable and conservative treatment options.
EchoSolv, the groundbreaking AI platform developed by Echo IQ, is revolutionizing the detection of aortic stenosis. With its unparalleled access to extensive echocardiographic data and AI-driven analysis, EchoSolv empowers clinicians to identify aortic stenosis earlier and with greater accuracy.
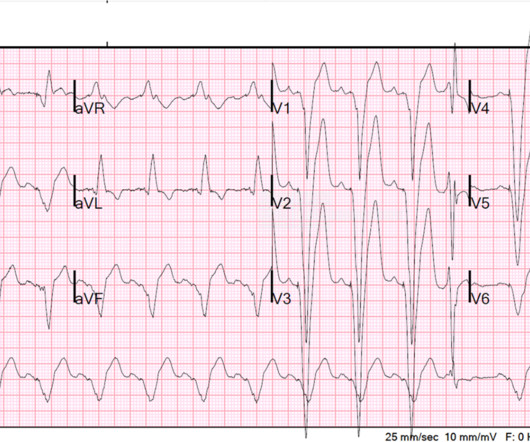
An undergraduate (not yet in medical school) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly arrived at work and happened to glance down and see this previously recorded ECG on a table in the ED. It was recorded at 0530: What do you think?
A normal functioning aortic valve has three leaflets, usually referred to as cusps, and is positioned at the end of the left ventricle. An aortic valve replacement is required if someone suffers from Aortic Valve Stenosis or Aortic Valve Insufficiency. That’s a reasonable question!
Date Nov 7, 2024 Image Blog Giving Credit Matters. Image Blog Managing Relationships with Patients Early career cardiothoracic surgeons have many important relationships that need to be managed and developed. Here's How to Do It.
Two weeks ago he had a significant MVC with many severe injuries, including aortic injury s/p endovascular repair. The clinical reality is that the overwhelming majority of cases in Dr. Smith's ECG Blog, in which acute pericarditis is strongly considered as the diagnosis based on ECG findings — turn out not to be the result of pericarditis.
If you’ve been diagnosed with aortic stenosis, you might have come across the term TAVR. our blog aims to clearly outline this procedure and how it can significantly improve your quality of life. Understanding Aortic Stenosis The aortic valve regulates blood flow from your heart’s main pumping chamber to the rest of your body.
Smith comment: Go here for a comprehensive blog post on syncope and link to the most detailed version of the Canadian Syncope Rule: Emergency Department Syncope Workup. See these blog posts. EMS reports intermittent sinus tachycardia and bradycardia secondary to some type of heart block during transport.
Written by Pendell Meyers A woman in her 20s with connective tissue disorder and history of aortic root and valve repair presented with palpitations. Further history revealed she had new onset atrial flutter soon after her aortic surgery, and was put on flecainide approximately 1 month ago. Here is her triage ECG: What do you think?
This was sent by an undergraduate (not yet in medical school, but applying now) who works as an ED technician (records all EKGs, helps with procedures, takes vital signs) and who reads this blog regularly. Edited by Smith He also sent me this great case.
The aortic valve is the largest of the heart's 4 valves and controls how blood is pumped from the left ventricle into the aorta. Learn how to keep it healthy.
Another possible cause of pseudonormalization of T waves mentioned many times on this blog is the pseudonormalization caused by re-occlusion of an infarct related reperfused coronary artery. Since serial ECGs are not available so either of the two patterns described above could be present (only serial ECG could differentiate).
Post PCI an intra-aortic balloon pump (IABP) was placed and a combination of norepinephrine and dobutamine was needed to maintain perfusion pressures. The image quality is not the best, but you can see the subtotal occlusion of the left main artery. Below is a still image with the red arrow indicating the subtotal LMCA stenosis.
Angiogram: Severe 95% hazy distal LM Severe 80% ostial LAD, 100% occluded distal LAD thought to be due to distal embolization from the lesion in the proximal LAD.
In this ECG Cases blog we look at 10 cases of patients with chest pain, including false positive STEMI, false negative STEMI, and other causes to help hone your ECG interpretation skills in time-sensitive cases where those very ECG skills might save a life.
The next morning the patient went for his routine echocardiogram, where the operator noticed a dilated aortic root at 5.47 cm with severe aortic insufficiency. The team was notified and they ordered a stat aortagram which showed type A aortic dissection from the aortic valve to the iliacs.
Many huge thanks to the entire EM Cases team, Advisory Board, SREMI, the amazing guest experts and you, the listeners of the podcasts, readers of the blogs, viewers of the videos and participants in the course, for making 2017 another successful year for EM Cases! And here they are.
The Midwest company will begin offering EchoSolv, an artificial intelligence clinical decision support platform designed to help detect severe aortic stenosis, to providers throughout the country. Omaha, Neb. –
I've copied KEY points from My Comment in the August 6, 2022 post in Dr. Smith's ECG Blog — regarding the answer to this question. Figure-1: The initial ECG in today's case. What are the ECG Findings of Cardiac Contusion? The ECG is less than optimally sensitive for detecting cardiac injury following blunt trauma.
Look at the aortic outflow tract. The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aortic valve. Aortic angiogram did not reveal aortic dissection. In fact, bedside ultrasound might even find severe aortic stenosis. What do you see?
If you don’t know the answers to these questions, then this is blog is going to answer all of your questions about the heart’s structure. The aortic semilunar valve is between the left ventricle and the aorta. However, not everyone knows much about the actual the heart’s structure. What are the major arteries and veins?
A dissection flap is noted in the intrabdominal aorta, and the aortic outflow tract is also noted to appear wider than normal. The CT angio showed a type A aortic dissection extending from the aortic root proximally to the carotid and left subclavian artery and distally to the common femoral arteries.
Like other cases on this blog who died before cath was done, I cannot prove that this patient had OMI. We have countless cases of missed posterior MI on this blog, including these: Interventionalist at the Receiving Hospital: "No STEMI, no cath. He was admitted to the cardiology floor and diagnosed with an NSTEMI. Were they right?
An echocardiogram confirmed aortic stenosis with a large pressure gradient. Now there is much less ST segment deviation, less elevation and less depression. The troponin returned positive, and the maximum troponin was 3.8 The next day, and angiogram showed normal coronary arteries. He awoke and did well.
The first troponin returned at 0.099 ng/mL (elevated, consistent with Non-Occlusion MI) Providers were concerned with aortic dissection, so they order a chest aorta CT. Here is here initial ECG: There is only a nonspecific flat T-wave in aVL. It is essentially normal.
At that previous visit, he had had some mildly elevated troponins, but mostly had severe heart failure from very poor systolic function and aortic stenosis. He has had previous angiograms showing "large vessels" and "no significant coronary disease." LV Ejection Fraction at the time of this hospitalization was 10%.
While the first one may radiate to the axilla and base, but usually not into the neck, it does reflect both aortic outflow obstruction and mitral regurgitation in patients with a large gradient. On the other hand, the murmur in valvular aortic stenosis does not change substantially or decreases slightly following the Valsalva maneuver.
2 cases of Aortic Stenosis: Diffuse Subendocardial Ischemia on the ECG. We’ve presented many variations on this theme on Dr. Smith’s Blog — with today’s case being distinguished by its discovery on abdominal exam ! Widespread ST-depression with reciprocal aVR ST-elevation can be cause by: Heart rate related: tachyarrhythmia (e.g.,
Today, for the third blog of this series, Global Cardiac Surgery is featuring Vietnam, a lower-middle-income country in Southeast Asia with a long standing experience and leading example for cardiac surgery in the Region. In addition, several centers are now performing minimally invasive aortic and mitral valve procedures with good results.
Due to the severity of the pain and the high BP, they obtained an aortic dissection CT. For more on the Mirror Test for recognizing posterior OMI — See My Comment in the September 21, 2022 post in Dr. Smith's ECG Blog ). especially since this Chest CT was done to rule out aortic dissection ).
Cardiology noted there was no STEMI criteria and the first troponin was in the normal range (25ng/L, with normal <26), so alternate diagnoses were considered and the patient was sent for CT to rule out aortic dissection. Selected LINKS on this Topic: ECG Blog #246 — Reviews the concept of the "Mirror Test" with a clinical example.
This is another case written by Pendell Meyers (who is helping to edit the blog and has many great recent posts) Case A 45 year old man was driving to work when he experienced acute onset sharp left sided chest pain with paresthesias of the left arm. On arrival his BP was 70s/40s, so an intra-aortic ballon pump was placed.
Given radiation of pain into the patient's back, he underwent CTA which showed no evidence of aortic dissection or any other acute pathology. By definition , this is acute myocardial infarction, the only question now is the etiology.
They also wanted an aortic CT which was negative. The chart says that "Cardiology agrees that the first ECG is early repolarization and similar to previous," but recommended giving aspirin and starting heparin and to wait for the first troponin to discuss. This is a "Transient OMI".
The estimated left ventricular ejection fraction is 58 % Aortic stenosis, mild, 9.0 The patient thus did not need immediate angiography. An echocardiogram showed: Left ventricular hypertrophy concentric. mmHg mean gradient. cm^2 valve area.
The patient had no hypertension, no tachycardia, a normal hemoglobin, no drug use, no hypotension/shock, no murmur of aortic stenosis. We also looked at his aortic root by both parasternal and suprasternal views, and the aorta was normal.]
As we've discussed on numerous other posts in Dr. Smith's ECG Blog ( See My Comment at the bottom of the page in the May 5, 2022 post) — a growing number of conditions other than Brugada Syndrome have been found to temporarily produce a Brugada-1 ECG pattern. What are the ECG Findings of Cardiac Contusion?
No signs for aortic dissection or pulmonary embolus. --"Results were discussed with the ordering physician. A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD LAD plaque with 0-25 percent stenosis. CAD-RADS category 1. --No
The patient arrived looking like an aortic dissection patient, so CTA was done and negative." ST elevation at 60 ms after the J-point in lead V3 = 1.5 mm Value using 400 ms QTc = 18.83 (significantly higher than 18.2 and thus indicating LAD occlusion). This all suggests a wraparound type III LAD to the inferior wall.
CT Aortogram revealed: No pulmonary embolism, No aortic dissection. Therefore, a patient with persistent pain and a troponin at this level has Acute MI with ongoing ischemia and should go to the cath lab regardless of the ECG (this is by American and European guidelines).
CT angiogram chest: no aortic dissection or pulmonary embolism. That said — acute MI does occur in younger patients ( witness the case referred to above by Dr. Smith — as well as the links from Dr. Meyers at the end of his discussion that refer to multiple cases published on Dr. Smith’s ECG Blog of young adults with acute MI ).
Blunt cardiac injury my result in : 1) Acute myocardial rupture with tamponade 2) Valve rupture (tricuspid, aortic, mitral) 3) Coronary thrombosis or dissection (and thus Acute MI) from direct coronary blunt injury 4) Dysrhythmias of all kinds.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content