This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Shettys team followed 252 patients who underwent the Ross procedure, a heart valve replacement operation commonly used to treat younger patients with severe aorticvalve disease. Three patients underwent the Ross-Konno procedure, in which the left-sided outflow root is enlarged to fit the pulmonary autograft. at 20 years.
Photo courtesy of Mount Sinai Health System milla1cf Thu, 02/22/2024 - 13:47 February 22, 2024 — Ismail El-Hamamsy , MD, PhD, Director of Aortic Surgery for the Mount Sinai Health System and the Mount Sinai Randall B. The aorticvalve controls blood flow from the heart into the aorta, the main artery that feeds blood to most of the body.
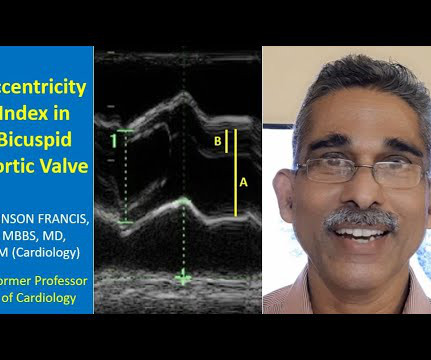
Transcript of the video: Closure line of aorticvalve on M-Mode echocardiogram, is seen as central line, while in bicuspid aorticvalve, it is an eccentric closure, nearer to one of the walls of the aorta. That is an important feature of bicuspid aorticvalve on M-Mode echocardiogram. This is a closure line.
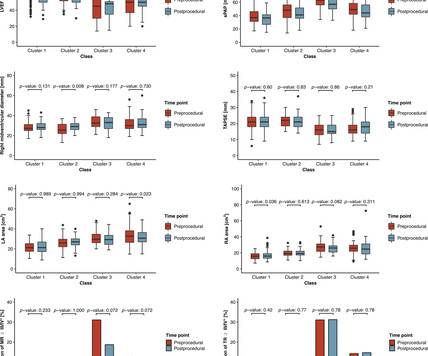
Objective A novel artificial intelligence-based phenotyping approach to stratify patients with severe aortic stenosis (AS) prior to transcatheter aorticvalve replacement (TAVR) has been proposed, based on echocardiographic and haemodynamic data. ±15.8 ±15.1 mm Hg, p value: 0.0079).
Pulmonary hypertension (PH) is a complex and progressive disorder characterised by elevated pulmonary artery pressure. Transcatheter aorticvalve implantation (TAVI) is a minimally invasive surgical procedure that has revolutionised the treatment of severe aortic stenosis (AS).
BackgroundChronic inflammatory disease (CID) accelerates atherosclerosis and the development of aortic stenosis. Data on long‐term outcomes after transcatheter aorticvalve implantation (TAVI) in those patients are missing. and 1.62, respectively).
Objective The European Society of Cardiology guidelines have recently defined new cut-offs for pulmonary hypertension (PH) and pulmonary vasculature resistance (PVR; median pulmonary artery pressure (mPAP) >20 instead of 25 mm Hg and PVR >2 instead of 3 Wood unit). Overall median age was 82 years, while 55.3%
Edwards has entered into an agreement to acquire JenaValve Technology , a pioneer in the transcatheter treatment of aortic regurgitation (AR), a deadly disease that impacts a significant and growing population and is largely untreated today. JenaValve presented positive results of its U.S. JenaValve presented positive results of its U.S.
The Ross procedure is a complex operation designed to replace a diseased or damaged aorticvalve. This unique surgery relies on a patient’s own existing tissue, the pulmonaryvalve, to replace the aorticvalve rather than using an artificial valve.
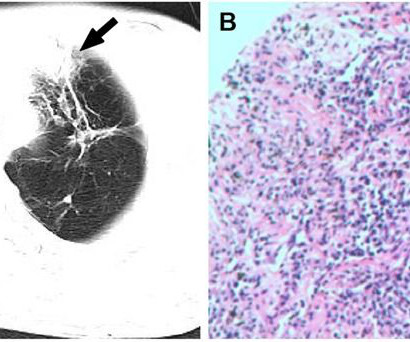
This report delineates two instances of AAV with large arterial involvement, one case presenting with lesions of the aorticvalve and the other with lesions of the pulmonary artery. The patient's aorticvalve thickening virtually disappeared after treatment with hormones combined with immunosuppressive agents.
Objectives This study aimed to evaluate the prognostic value of coronary microvascular dysfunction (CMD) at long term after transcatheter aorticvalve implantation (TAVI) and to explore its relationship with extravalvular cardiac damage (EVCD). CMD was defined as IMR angio ≥30 units.
Pulmonary hypertension patients who undergo transcatheter aorticvalve replacement are at a higher risk for mortality than those without pulmonary hypertension, according to a recent study.
Clinical introduction A patient in their 30s had been diagnosed with peripartum cardiomyopathy, pulmonary oedema, with severe left ventricular dysfunction at the seventh month of gestation in the third pregnancy in their late 20s. The patient had pregnancy-induced hypertension and hypothyroidism and was treated accordingly.
Patients with significant pulmonary oedema or aorticvalve (AV) closure during venoarterial extracorporeal membrane oxygenation (VA-ECMO) were randomized to early left ventricular (LV) unloading or conventional strategy groups (1:1). The primary endpoint was the rate of weaning from VA-ECMO during index admission. vs. 1.7 ± 0.6
Transcript of video: Hypoplastic Left Heart Syndrome is a very severe form of congenital heart disease, in which, the left ventricle, aorta and mitral and aorticvalves are hypoplastic and valves may be atretic as well. So right ventricle maintains both systemic and pulmonary circulation after a Norwood procedure.
Assessment of fluid overload identifies aortic stenosis (AS) patients at high risk and treatment of fluid overload may potentially improve the post-interventional clinical course. TAVI, transcatheter aorticvalve implantation. FO by BIS was defined as ≥1.0 L L = euvolaemia). FO by BIS was defined as ≥1.0 L L = euvolaemia).
Pulmonary vein isolation (PVI) is a well-established therapy for treating AF, but performing PVI in patients with known LAA thrombus is contraindicated. Cerebral protection devices (CPDs) are routinely used to capture and remove thrombus/debris during transcatheter aorticvalve replacement procedures.
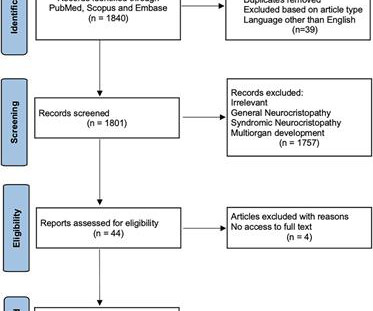
Cardiovascular neurocristopathy, i.e., cardiopathy and vasculopathy, associated with the NCC could occur in the form of (1) cardiac septation disorders, mainly the aortico-pulmonary septum; (2) great vessels and vascular disorders; (3) myocardial dysfunction; and (4) a combination of all three phenotypes.
I've previously discussed the interesting correlation of a qR pattern in lead V1 in patients with RVH — as strongly suggesting associated pulmonary hypertension ( See ECG Blog #234 and Blog #248 ). The plan was to proceed as soon as possible with aorticvalve replacement. E CG F indings in Today's Tracing N ow M ake S ense !
This year's Boot Camp covered training in cardiopulmonary bypass skills, vessel anastomosis, diagnostic and therapeutic endoscopies, open pulmonary lobectomy, TAVR, and wire skills.
This is the aorticvalve in closed position and mitral valve also appears to be closed in position. That is because timing of the image may be in such a way that, it could have been in such a way that both valves are in closed position. You can also see the aortic override. Right ventricle, left ventricle.
Written by Pendell Meyers A woman in her 20s with connective tissue disorder and history of aortic root and valve repair presented with palpitations. Further history revealed she had new onset atrial flutter soon after her aortic surgery, and was put on flecainide approximately 1 month ago. Atrial flutter with 2:1 conduction.
Look at the aortic outflow tract. The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aorticvalve. Aortic angiogram did not reveal aortic dissection. If you see this, you should Doppler the valve. What do you see?
The next morning the patient went for his routine echocardiogram, where the operator noticed a dilated aortic root at 5.47 cm with severe aortic insufficiency. The team was notified and they ordered a stat aortagram which showed type A aortic dissection from the aorticvalve to the iliacs.
Usual structures imaged in this view are the right ventricular free wall and outflow region, interventricular septum, aorta, and aorticvalve, left ventricular outflow tract, anterior and posterior mitral leaflets, left ventricular cavity, posterior wall of left ventricle and left atrium. Colour flow shows the flow in pulmonary artery.
We are blessed with 4 heart valves – 2 on the left side which are known as the mitral and aorticvalves and 2 on the right side – the tricuspid and pulmonaryvalves.
BACKGROUND:Recent guidelines redefined exercise pulmonary hypertension as a mean pulmonary artery pressure/cardiac output (mPAP/CO) slope >3 mm Hg·L−1·min−1. Peak aortic velocity (odds ratio [OR] per SD, 1.48;P=0.036), Peak aortic velocity (odds ratio [OR] per SD, 1.48;P=0.036),
Objective Patients with low-flow, low-gradient aortic stenosis (LFLG AS) and reduced left ventricular ejection fraction (LVEF) are known to suffer from poor prognosis after transcatheter aorticvalve implantation (TAVI). This study aimed to develop a simple score system for risk prediction in this vulnerable subset of patients.
Venn diagram highlighting the main similarities and differences between heart failure with preserved ejection fraction (HFpEF) and aortic stenosis with preserved ejection fraction (ASpEF). Patients with ASpEF eligible for transcatheter aorticvalve replacement ( n = 125) also performed cardiac computed tomography (CT).
Objective To characterise the mechanics responsible for the reduced ejection fraction (rEF) in high-gradient severe aortic stenosis (AS). Methods 21 patients with high-gradient severe AS (aorticvalve area (AVA) <1.0 mm Hg/mL; p=0.05), driven by higher degrees of valvular stenosis (valve area 0.46 N/cm 2 ; p<0.01
By these mechanisms, SMC-MR promotes disease progression in models of aging-associated vascular stiffness, vascular calcification, mitral and aorticvalve disease, pulmonary hypertension, and heart failure. While rarely tested, when sexes were compared, the mechanisms of SMC-MR-mediated disease were sexually dimorphic.
Program Designations Access and Publications (A&P) 1 Participant User File (PUF) 2 Task Force on Funded Research (TFR) 3 Special Projects 4 Adult Cardiac Surgery Database Lead Author Title Publication Date William Keeling 2 National Trends in Emergency Coronary Artery Bypass Grafting European Journal of Cardiothoracic Surgery October 2023 Jake (..)
I suspect pulmonary edema, but we are not given information on presence of B-lines on bedside ultrasound, or CXR findings. Anything that causes pulmonary edema: poor LV function, fluid overload, previous heart failure (HFrEF or HFpEF), valvular disease. What "initiates" the aortic stenosis cascade? She was started on lasix.
Larger shunt volume means less blood exiting the left ventricle through the aorticvalve and lower cardiac output. Rupture can be either free wall rupture (causing tamponade) or septal rupture, causing ventricular septal defect with left to right flow and resulting pulmonary edema and shock.
AF, atrial fibrillation; LAVI, left atrial volume index; RA, right atrial; RV, right ventricular; sPAP, systolic pulmonary artery pressure; SVI, stroke volume index; TR, tricuspid regurgitation. Aims Paradoxical low-flow, low-gradient aortic stenosis (pLFLG AS) may represent a diagnostic challenge, and its pathophysiology is complex.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





































Let's personalize your content