This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Background Heart failure with preserved ejection fraction is a recognised outcome in patients with myocardialinfarction, although heart failure with reduced ejection fraction is more common. Among patients with myocardialinfarction, a 1-SD increase in pulse pressure was associated with a 1.60-fold m/s had a 2.10-fold
Heart failure (HF) is one of the significant complications in patients with myocardialinfarction (MI), leading to increased risk for cardiovascular morbidity and mortality. 2 However, mortality rate is greater in HF cases developing >3 days following MI compared with less than or equal to 3 days after MI.
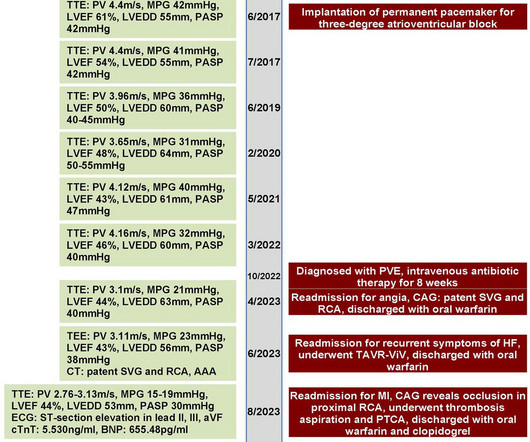
A 70-year-old female patient with a history of bioprosthetic aorticvalve replacement and coronary artery bypass graft presented with bioprosthetic valve failure secondary to prosthetic valve endocarditis. This resulted in early death due to myocardialinfarction and acute heart failure.
Small aortic annulus poses a major challenge in aorticvalve replacement due to the increased risk of prosthesispatient mismatch (PPM) and increased surgical risk. In recent years, transcatheter aorticvalve replacement (TAVR) has emerged as a popular alternative to the traditional surgical aorticvalve replacement.
The NOTION trial, a pioneering study, sought to compare the long-term clinical and bioprosthesis outcomes of Transcatheter AorticValve Implantation (TAVI) versus Surgical AorticValve Replacement (SAVR) in patients with severe aorticvalve stenosis (AS) at lower surgical risk.
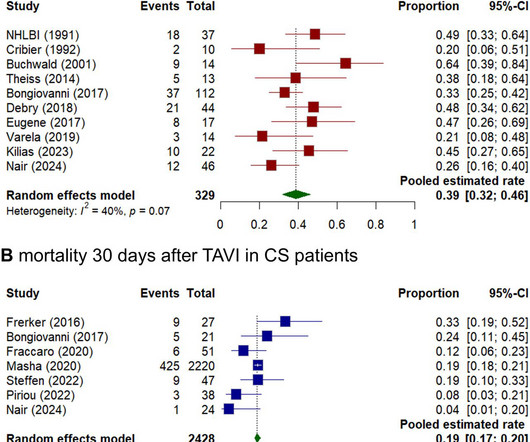
Background Cardiogenic shock (CS) induced by severe aortic stenosis (AS) is a life-threatening condition with high mortality. Aim This study aimed to systematically review and analyse the existing evidence on outcomes of emergency transcatheter aorticvalve implantation (eTAVI) and emergency balloon aortic valvuloplasty (eBAV) in CS patients.
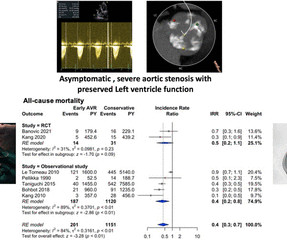
Background A quarter of patients with severe aortic stenosis (AS) were asymptomatic, and only a third of them survived at the end of 4 years. Only a select subset of these patients was recommended for aorticvalve replacement (AVR) by the current American College of Cardiology/American Heart Association guidelines.
Prosthetic valve thrombosis (PVT) in aorticvalve and its complication coronary embolism is a very rare condition. We present a young patient with acute myocardi. Diagnosis and treatment process is challenging.
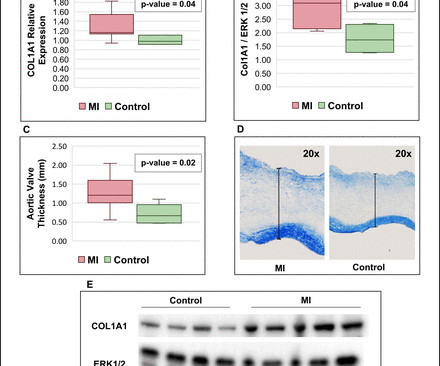
Background Myocardialinfarction (MI) has been shown to induce fibrotic remodelling of the mitral and tricuspid valves. It is unknown whether MI also induces pathological remodelling of the aorticvalve and alters aortic stenosis (AS) progression. vs –0.04±0.04 cm 2 /m 2 /year; p=0.004).
This study aimed to confirm the prognostic value of a novel angiographic microvascular resistance (AMR) index in patients undergoing transcatheter aorticvalve replacement.Methods and ResultsWe prospectively included 335 patients with severe aortic stenosis who underwent transcatheter aorticvalve replacement at Fuwai Hospital.
BackgroundLp(a) (lipoprotein(a)) is an independent risk factor for calcific aorticvalve stenosis (CAVS). Journal of the American Heart Association, Ahead of Print. Whether patients with CAVS and high Lp(a) levels are at higher risk of valvular or cardiovascular events is unknown.
BackgroundCurrent guidelines and expert consensus recommend lifelong single antiplatelet therapy for patients undergoing transcatheter aorticvalve replacement who have no indication for anticoagulation or dual antiplatelet therapy. Journal of the American Heart Association, Ahead of Print.
The kappa was higher in MA versus FFS for diabetes (P=0.03) and hypertension (P=0.025) but was lower in myocardialinfarction (P<0.0001). For the outcomes, sensitivities were 85% for bleeding (comprehensive), permanent pacemaker implantation, and death.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
Objective The optimal medical therapy after surgical aorticvalve replacement (SAVR) for aortic stenosis remains unknown. Methods All patients undergoing SAVR due to aortic stenosis in Sweden 2006–2020 and surviving 6 months after surgery were included.
Objective Postprocedural ischaemic and bleeding risks after transcatheter aorticvalve replacement (TAVR) remain a major concern. Ischaemic events were defined as myocardialinfarction, stroke, transient ischaemic attack or peripheral embolism at 1 year.
Background:Atherosclerotic cardiovascular disease (ASCVD) is highly prevalent in patients with severe aortic stenosis undergoing transcatheter aorticvalve replacement (TAVR). Circulation: Cardiovascular Interventions, Ahead of Print. Exposure of interest was PVD. Primary outcome was all-cause mortality.
This is a value typical for a large subacute MI, n ormal value 48 hours after myocardialinfarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). Mechanical complications secondary to myocardialinfarction are infrequent due to most patients receiving revascularization quite rapidly.
BACKGROUND:Food and Drug Administrationmandated postmarket studies for transcatheter aorticvalve replacement in low-risk populations plan to use passively collected registry data linked to claims for long-term follow-up out to 10 years. Circulation: Cardiovascular Interventions, Volume 18, Issue 1 , Page e014592, January 1, 2025.
First degree AV block can sometimes be a manifestation of diseases like rheumatic fever, a disease which affects predominantly the joints and the valves of the heart. First degree heart block can also occur in a heart attack involving the lower part of the heart known as inferior wall myocardialinfarction.
This typically occurs after an inferior posterior myocardialinfarction, drug-induced CHB. Management of conduction disturbances associated with transcatheter aorticvalve replacement: JACC Scientific Expert Panel. J Am Coll Cardiol. 2019; 74 : 1086-1106.
EMPACT-MI 1 ( NCT04509674 ) studied the effects of empagliflozin in patients who have experienced myocardialinfarction (MI). SMART 4 ( NCT04722250 ) studied patients with severe aortic stenosis and a small aortic annulus who underwent transcatheter aorticvalve replacement (TAVR).
While intracardiac cardiac tumors and shunts are infrequent and typically asymptomatic, their existence can precipitate severe outcomes, including stroke, myocardialinfarction and sudden death.Case Description:A 69-year-old female presented with left sided facial droop, slurred speech and left arm weakness.
Look at the aortic outflow tract. The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aorticvalve. Aortic angiogram did not reveal aortic dissection. If you see this, you should Doppler the valve. What do you see?
Objectives Grading the severity of moderate mixed aortic stenosis and regurgitation (MAVD) is challenging and the disease poorly understood. Methods Moderate MAVD was defined as coexisting moderate aortic stenosis (aorticvalve area (AVA) 1.0–1.5 cm 2 ) and moderate aortic regurgitation (vena contracta (VC) 0.3–0.6
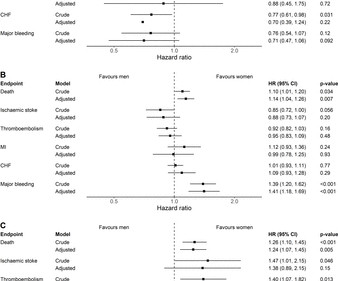
Objective To compare long-term cardiovascular (CV) outcomes between men and women with aortic stenosis (AS) undergoing aorticvalve replacement (AVR) by the type of valve implant. Conclusion No significant long-term difference in CV events was noted between men and women undergoing AVR with a mechanical aorticvalve.
Background and aims Randomised controlled trials comparing transcatheter aorticvalve replacement (TAVR) and surgical aorticvalve replacement (SAVR) were performed in highly selected populations and data regarding long-term secondary complications beyond mortality are scarce. to 1.43), 3 years (HR 1.45; 95% CI 1.28
Adult Cardiac Surgery Database Lead Author Title Publication Date Jacob Raphael Red Blood Cell Transfusion and Pulmonary Complications: The Society of Thoracic Surgeons Adult Cardiac Surgery Database Analysis The Annals of Thoracic Surgery January 2024 Joseph Sabik Multi-Arterial versus Single-Arterial Coronary Surgery: Ten Year Follow-up of One Million (..)
Program Designations Access and Publications (A&P) 1 Participant User File (PUF) 2 Task Force on Funded Research (TFR) 3 Special Projects 4 Adult Cardiac Surgery Database Lead Author Title Publication Date William Keeling 2 National Trends in Emergency Coronary Artery Bypass Grafting European Journal of Cardiothoracic Surgery October 2023 Jake (..)
It could also, given a different clinical context be compatible with a subacute myocardialinfarction complicated by post infarct regional pericarditis. Most common cause) 2 ) Post infarct regional pericarditis. Due to the atypical and vague symptoms, the myocardialinfarct was not initially diagnosed.
Aims Paradoxical low-flow, low-gradient aortic stenosis (pLFLG AS) may represent a diagnostic challenge, and its pathophysiology is complex. AF, atrial fibrillation; LAVI, left atrial volume index; RA, right atrial; RV, right ventricular; sPAP, systolic pulmonary artery pressure; SVI, stroke volume index; TR, tricuspid regurgitation.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






























Let's personalize your content