This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The Be Active Randomized Clinical Trial Zilebesiran in Combination with a Standard-of-care Antihypertensive in Patients With Inadequately Controlled Hypertension: Primary Results From the Phase 2 Kardia-2 Study Efficacy and Safety of Olezarsen in Patients with Hypertriglyceridemia and High Cardiovascular Risk: Primary Results of the BRIDGE-TIMI 73a (..)
Description of Case:A 64-year-old male with complex medical history, including infective endocarditis of the aorticvalve requiring surgical replacement with a bioprosthetic valve and recurrent infective endocarditis of the bioprosthetic valve, presented with two hours of crushing chest pain and found to have ST elevations.
Smith comment: This patient did not have a bedside ultrasound. Had one been done, it would have shown a feature that is apparent on this ultrasound (however, this patient's LV function would not be as good as in this clip): This is recorded with the LV on the right. Look at the aortic outflow tract. What should be done?
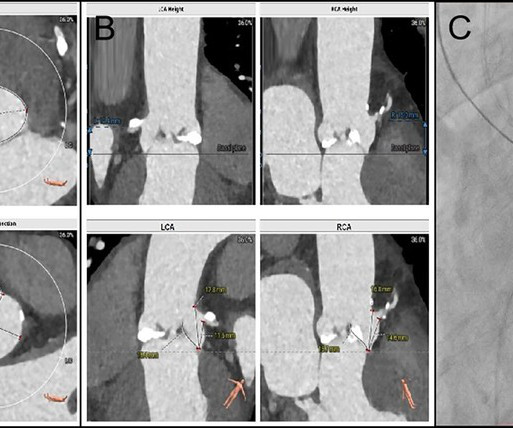
BackgroundFollowing transcatheter aorticvalve replacement, acute coronary obstruction is infrequent but potentially life-threatening, while delayed coronary obstruction is even more uncommon.Case summaryA 69-year-old male underwent TAVR and subsequently developed an acute obstruction in the left main coronary artery.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










Let's personalize your content