This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Transcatheter aorticvalve replacement (TAVR) has become a leading treatment for aorticstenosis, but managing thromboembolic and bleeding risks post-procedure remains challenging. This review examines current evidence on antithrombotic therapy after TAVR.
ObjectivesRegistered, prospective, multicenter study of the short-term clinical outcomes of a novel transcatheter aorticvalve system (Xcor system, Saint Medical Technology, Inc., Procedural, in-hospital, and follow-up clinical outcomes were evaluated after procedures.ResultsThe average age of the 130 patients was 71.24.4
tim.hodson Mon, 03/31/2025 - 15:39 March 30, 2025 Medtronic has announced late-breaking data on five-year outcomes from the Evolut Low Risk Trial. The lower mortality risk and strong valve performance is meaningful for clinicians in evaluating treatment approaches that prioritize the overall well-being of patients." Reardon, M.D.,
Valvular heart disease, including calcific or degenerative aorticstenosis (AS), is increasingly prevalent among the older adult population. Over the last few decades, treatment of severe AS has been revolutionised following the development of transcatheter aorticvalve replacement (TAVR).
IntroductionSince TAVR was approved for lower-risk aorticstenosis (AS) patients, managing post-implantation conduction disturbances has become crucial, especially with self-expanding heart valves (SEV). Forty-seven received SEVs using COL, and 50 with CON techniques.
Getty Images milla1cf Mon, 01/29/2024 - 14:24 January 29, 2024 — Despite national guidelines recommending surgical aorticvalve replacement (SAVR) for patients under age 65 with severe aorticstenosis , many hospitals are still opting for a nonsurgical approach in patients under 60—possibly with poorer survival rates.
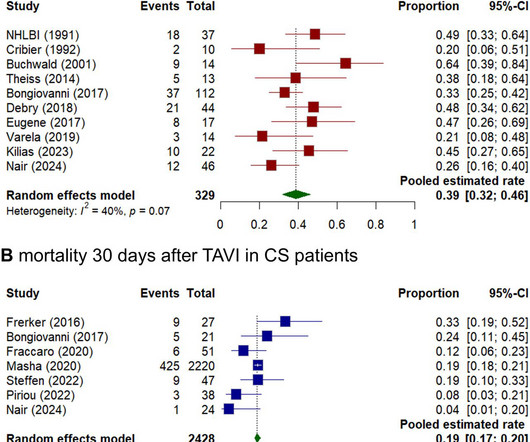
Background Cardiogenic shock (CS) induced by severe aorticstenosis (AS) is a life-threatening condition with high mortality. Despite advancements in emergency interventions, the optimal treatment approach remains uncertain.
Objectives The clinical outcomes of transcatheter aorticvalve replacement (TAVR) in patients with aorticstenosis (AS) and concomitant active cancer remain insufficiently explored. This study aimed to assess the midterm outcomes of TAVR in patients diagnosed with AS and active cancer.
Transcatheter aorticvalve replacement (TAVR) is the standard treatment for severe aorticstenosis, but post-TAVR leaflet thrombus, identified by hypoattenuated leaflet thickening (HALT), poses potential risks like cerebral thromboembolic events. had thrombus at any aorticvalve complex. Specifically, 14.2%
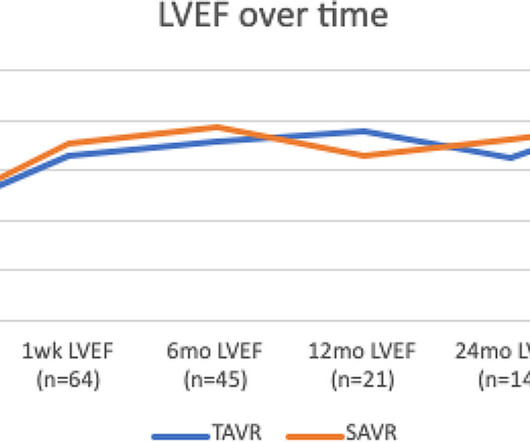
Patients with severe aorticstenosis (AS) and left ventricular (LV) dysfunction demonstrate improvement in left ventricular injection fraction (LVEF) after aorticvalve replacement (AVR). The timing and magnit.
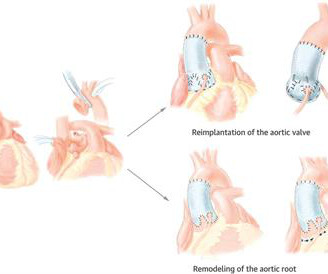
Bicuspid aorticvalve (BAV) is a common congenital heart condition that can lead to some valve-related complications, such as aorticstenosis and/or regurgitation, and is often associated with aortic root dilation.
The goal of the NOTION trial was to compare outcomes after transcatheter aorticvalve replacement (TAVR) versus surgical aorticvalve replacement (SAVR) in unselected patients with severe degenerative aorticstenosis.
Transcatheter aorticvalve replacement (TAVR) is a relatively new treatment method for aorticstenosis (AS) and has been demonstrated to be suitable for patients with varying risk levels.
Surgical aorticvalve replacement (SAVR) is an established therapy for severe calcific aorticstenosis. Enhanced recovery after cardiac surgery (ERACS) protocols have been shown to improve outcomes for electiv.
Some patients with aorticstenosis may require multiple valve interventions in their lifetime, and choosing transcatheter aorticvalve replacement (TAVR) as the initial intervention may be appealing to many. If their transcatheter heart valve degenerates later in life, most will hope to undergo redo-TAVR.
BACKGROUND:Data concerning the outcomes of transcatheter aorticvalve replacement in type 0 bicuspid aorticstenosis (AS) are scarce. Self-expanding transcatheter heart valves were used in the majority of patients (n=1160; 91.4%). Circulation: Cardiovascular Interventions, Ahead of Print.
What are the hemodynamic and clinical outcomes after transcatheter aorticvalve replacement (TAVR) and surgical aorticvalve replacement (SAVR) among patients with severe aorticstenosis (AS) and a small aortic annulus?
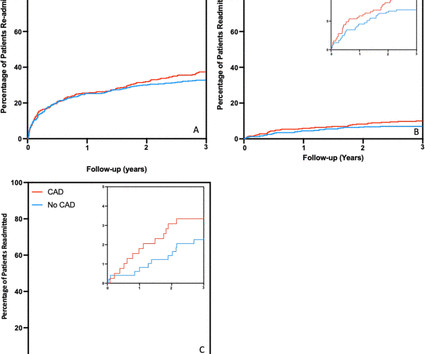
Background Aorticstenosis is a life-limiting condition for which transcatheter aorticvalve implantation (TAVI) is an established therapy. Subsidiary outcomes included patient angina and breathlessness scores. After multivariate analysis, the presence of CAD had no effect on the primary outcome (HR 0.98, CI 0.68
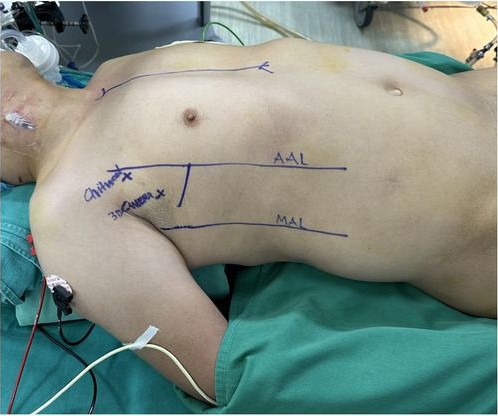
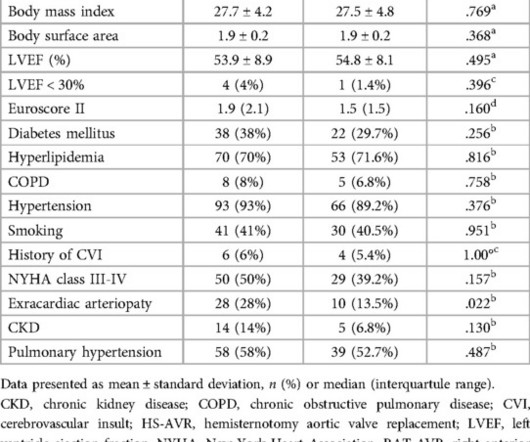
Patient selection was based on the presence of isolated aorticvalve disease without the need for ascending aorta replacement or aortic root enlargement. The majority of patients (77.1%) presented with aorticstenosis, often accompanied by severe calcification. years, with 22.9% being female.
This concept should be applied when managing older patients with severe aorticstenosis. Although left ventricular wall hypertrophy is expected in patients with aorticstenosis, it should not be assumed that this is caused only by aorticstenosis.
He then discusses a recent paper investigating the superiority of transcatheter aorticvalve implantation (TAVI) to surgical aorticvalve replacement (SAVR) at one year in women with severe aorticstenosis (AS).
BACKGROUND:This study aimed to compare the incidence and prognostic implications of new-onset conduction disturbances after surgical aorticvalve replacement (SAVR) in patients with bicuspid aorticvalve (BAV) aorticstenosis (AS) versus patients with tricuspid aorticvalve (TAV) AS (ie, BAV-AS and TAV-AS, respectively).
ConclusionAortic valve replacement with the Perceval S valve through either an upper hemisternotomy or a right anterior thoracotomy is a procedure associated with low perioperative complication rates. This was a retrospective, single-center observational study. ResultsThe overall in-hospital mortality was 1,7%.
BackgroundAortic stenosis has pathophysiological similarities with atherosclerosis, including the deposition of cholesterol‐containing lipoproteins. Journal of the American Heart Association, Ahead of Print. In multivariate analysis, low CCDR (hazard ratio, 2.21 [95% CI, 0.99–4.92],P=0.04)
BackgroundAortic stenosis can lead to cardiac adaptations and symptoms similar to heart failure with preserved ejection fraction. Methods and ResultsThis retrospective cohort study included 469 patients with moderate aorticstenosis. versus 4.4 m/s in patients with a low H2FPEF score (P<0.001).
Morristown Medical Center’s Gagnon Cardiovascular Institute’s structural heart program recently reported it has reached a significant milestone of performing over 5,000 transcatheter aorticvalve replacement (TAVR) procedures, the first in New Jersey and among the first to accomplish this in the United States.
BACKGROUND:Patients with paradoxical low-flow, low-gradient severe aorticstenosis exhibit low transvalvular flow rate (Q), while maintaining preserved left ventricular ejection fraction. Over a follow-up of up to 5 years, severe MR correlated with higher all-cause mortality (P=0.02) and aorticvalve replacement rates (P=0.012).
Objective To investigate the impact of prior coronary artery bypass grafting (CABG) and coronary lesion complexity on transcatheter aorticvalve replacement (TAVR) outcomes for aorticstenosis. 23), which was not associated with better/worse clinical outcomes in patients with prior CABG.
BackgroundChronic inflammatory disease (CID) accelerates atherosclerosis and the development of aorticstenosis. Data on long‐term outcomes after transcatheter aorticvalve implantation (TAVI) in those patients are missing. Long‐term (up to 5 years) clinical and echocardiographic outcomes were studied.
Aorticstenosis (AS) due to fibrosis and calcification of the aorticvalve is a hazardous component of cardiovascular disease burden—after developing symptomatic AS, patients survive for an average of less than 2 years without treatment.
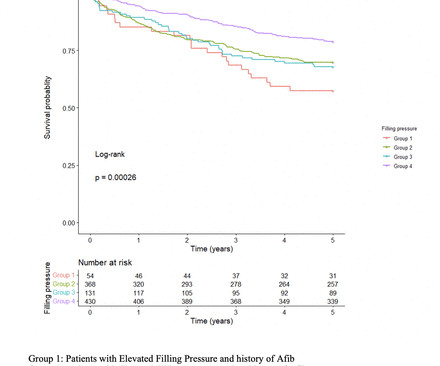
Background Increase in left ventricular filling pressure (FP) and diastolic dysfunction are established consequences of progressive aorticstenosis (AS). However, the impact of elevated FP as detected by pretranscatheter aorticvalve replacement (TAVR) echocardiogram on long-term outcomes after TAVR remains unclear.
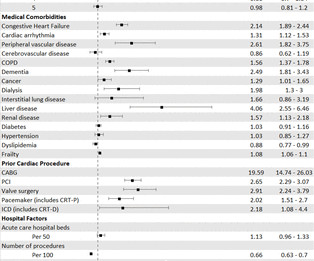
Objectives To understand the patient and hospital level drivers of the variation in surgical versus trascatheter aorticvalve replacement (SAVR vs TAVR) for patients with aorticstenosis (AS) and to explore whether this variation translates into differences in clinical outcomes.
ABSTRACT Patients with severe aorticstenosis (AS) may develop heart failure (HF), the presence of which has traditionally been deemed as a final stage in AS progression with poor outcomes. The use of transcatheter aorticvalve replacement (TAVR) has become the preferred therapy for most patients with AS and concomitant HF.
Aorticvalvestenosis (AS) is often a contraindication to liver transplantation (LT). Despite the widely accepted impact of liver cirrhosis on aorticvalve hemodynamics, the change in these parameters with LT or impact of AS on LT outcomes has not been described.
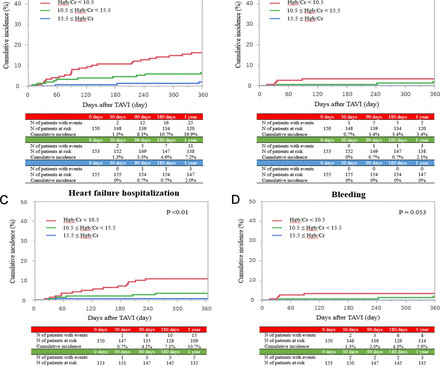
Objective The association between a combined anaemia and renal failure index and 1-year prognosis of patients undergoing transcatheter aorticvalve implantation (TAVI) is unexplored. The primary clinical outcome measure was all-cause mortality and heart failure hospitalisation 1 year after TAVI.
A new study demonstrates parity between a minimally invasive procedure to replace the aorticvalve in the heart—transcatheter aorticvalve replacement (TAVR)—and surgical aorticvalve replacement (SAVR).
What are clinical outcomes among patients with severe aorticstenosis (AS) and coronary artery disease (CAD) undergoing surgical aorticvalve replacement (SAVR) plus revascularization versus transcatheter aorticvalve replacement (TAVR) plus percutaneous coronary intervention (PCI)?
Transcatheter aorticvalve replacement (TAVR) is increasingly being performed in younger and lower surgical risk patients. Reintervention for failed transcatheter heart valves will likely increase in the future as younger patients are expected to outlive the initial bioprosthesis.
Transcatheter aorticvalve replacement (TAVR) has increasingly become a safe, feasible, and widely accepted alternative surgical treatment for patients with severe symptomatic aorticstenosis.
Patients with bicuspid aorticvalves (BAV) are predisposed to the development of aorticstenosis. We performed a pairwise meta-analysis, comparing the efficacy of transcatheter aorticvalve replacement (TAVR) versus surgical aorticvalve replacement (SAVR) in patients with BAV.
Procedure trends certainly suggest that we’ve entered the TAVR era, but a pair of new studies show that surgical aorticvalve replacement (SAVR) is a far better option for many younger and healthier patients who are increasingly seen as TAVR candidates. The post SAVR’s Value in the TAVR Era appeared first on Cardiac Wire.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content