This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Transcript of the video: Closure line of aorticvalve on M-Mode echocardiogram, is seen as central line, while in bicuspid aorticvalve, it is an eccentric closure, nearer to one of the walls of the aorta. That is an important feature of bicuspid aorticvalve on M-Mode echocardiogram.
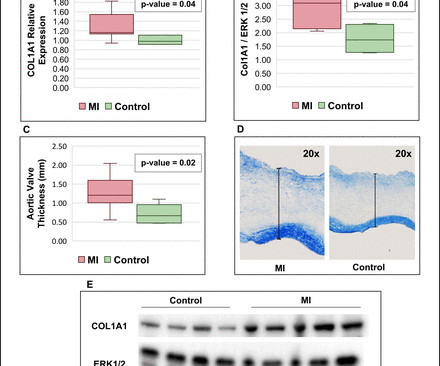
It is unknown whether MI also induces pathological remodelling of the aorticvalve and alters aorticstenosis (AS) progression. We thus compared AS progression after an acute MI and in patients with/without history of MI, and assessed post-MI pathobiological changes within the aorticvalve leaflets in a sheep model.
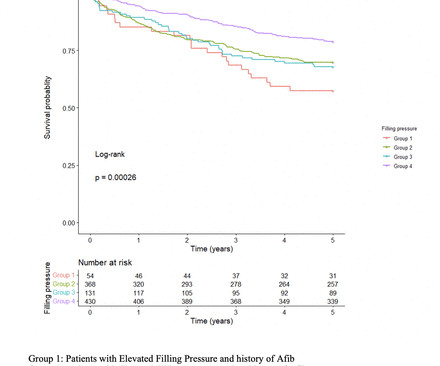
Background Increase in left ventricular filling pressure (FP) and diastolic dysfunction are established consequences of progressive aorticstenosis (AS). However, the impact of elevated FP as detected by pretranscatheter aorticvalve replacement (TAVR) echocardiogram on long-term outcomes after TAVR remains unclear.
Background:Peak aorticvalve Doppler velocity, mean aorticvalve gradient, and Doppler estimated aorticvalve area are key measures recommended for assessing aorticstenosis severity. Failure to accurately diagnose severe aorticstenosis is critical.
Background: Symptomatic severe aorticstenosis (AS) remains undertreated with high resultant mortality despite increased growth and availability of aorticvalve replacement (AVR) since the advent of transcatheter therapies. The patient cohort had mean age of 7711 years, was 47% female, and had mean aorticvalve area 0.80.1
Data from the studies demonstrated that AISAP CARDIO enables non-cardiologist physicians to interpret point-of-care echocardiograms just as well as expert cardiologists of the MGB echocardiography lab. James Hillis, MBBS, DPhil, director of Clinical Operations at Mass General Brigham AI.
Patent Foramen Ovale 4. Severe calcific Aortic (valve) Stenosis 5. Mechanical prosthetic valve Severe carotid artery stenosis is also implicated in embolic stroke.
The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aorticvalve. Aortic angiogram did not reveal aortic dissection. If you see this, you should Doppler the valve. In fact, bedside ultrasound might even find severe aorticstenosis.
Echocardiogram in parasternal long axis view shows dilated left ventricle, left atrium, aorta and a small portion of the right ventricle, which is usually the outflow region. Mitral valve leaflets seen in open position between the left ventricle and left atrium are thickened. Aorticvalve is seen as grossly thickened and calcified.
The image shown here is an animated 2 dimensional echocardiogram. This one is an older mode known as time-motion mode or M-Mode echocardiogram. Planimetry of mitral valve area can be obtained in parasternal short axis view in case of mitral stenosis. Exact position and angulation will vary between individuals.
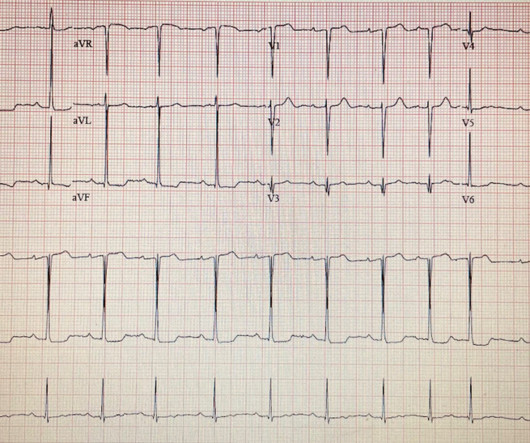
They found non-obstructive CAD, with only a 20% stenosis of OM2 and 10% RCA. The next morning the patient went for his routine echocardiogram, where the operator noticed a dilated aortic root at 5.47 cm with severe aortic insufficiency. A repeat ECG was performed and cardiology was re-consulted: Roughly unchanged.
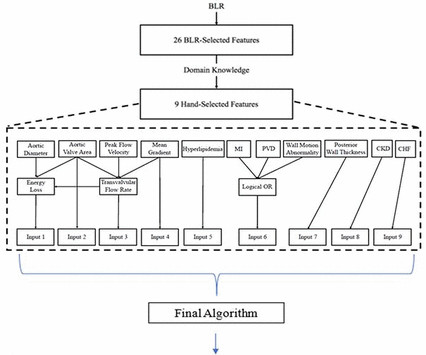
Objective To use echocardiographic and clinical features to develop an explainable clinical risk prediction model in patients with aorticstenosis (AS), including those with low-gradient AS (LGAS), using machine learning (ML). Our algorithm, the AorticStenosis Risk (ASteRisk) score, is available online for public use.
Objective We developed an artificial intelligence decision support algorithm (AI-DSA) that uses routine echocardiographic measurements to identify severe aorticstenosis (AS) phenotypes associated with high mortality. million echocardiograms were randomly spilt into two groups. Methods 631 824 individuals with 1.08
More troponin values were measured at the cardiac center: 2327- 267 ng/L 0821- 355 ng/L 1108- 305 ng/L An echocardiogram on day three of the patients admission showed an ejection fraction of 46% with abnormal basal inferior and basal lateral segments, and severe aorticstenosis. What "initiates" the aorticstenosis cascade?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content