This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
After 24 hours, the patient was readmitted to the hospital with chestpain and troponin elevation, without ECG changes. A transthoracic echocardiogram (TTE) revealed a mobile mass on the right coronary cusp of the aorticvalve ( figure 1 , ). Figure 1 A mobile mass (1.88
Submitted and written by Quinton Nannet, MD, peer reviewed by Meyers, Grauer, Smith A woman in her 70s recently diagnosed with COVID was brought in by EMS after she experienced acute onset sharp midsternal chestpain without radiation or dyspnea. Intraoperative TEE noted "Type A aortic dissection arising 1.0
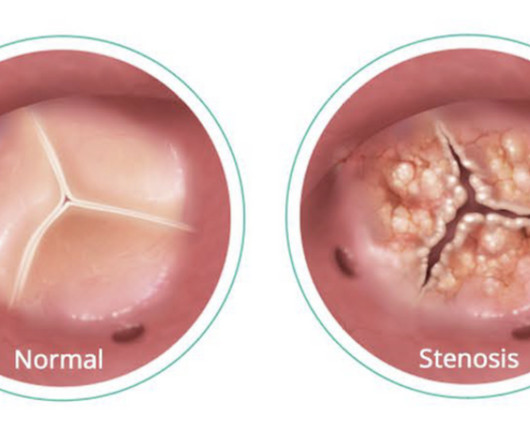
Understanding Aortic Stenosis The aorticvalve regulates blood flow from your heart’s main pumping chamber to the rest of your body. In aortic stenosis, the valve leaflets stiffen and narrow, restricting blood flow. A Closer Look at Transcatheter AorticValve Replacement appeared first on AMS Cardiology.
Left ventricular afterload reduction is essential to decrease the trans-se ptal pressure gradient and thus decrease shunt volume, making a larger proportion of the blood flow from the left ventricle through the aorticvalve. Not all patients with acute ( or recent ) MI have chestpain with their event.
ET Murphy Ballroom 4 ACC.24 24 planners note that attendees can gain insights from key clinical trials presented at ACC.24 24 and how those may impact clinical practice and patient care in this deep dive clinical trial session.
Description of Case:A 64-year-old male with complex medical history, including infective endocarditis of the aorticvalve requiring surgical replacement with a bioprosthetic valve and recurrent infective endocarditis of the bioprosthetic valve, presented with two hours of crushing chestpain and found to have ST elevations.
Written by Pendell Meyers A man in his late 40s with several ACS risk factors presented with a chief complaint of chestpain. Several hours prior to presentation, while driving his truck, he started experiencing new central chestpain, without radiation, aggravating/alleviating factors, or other associated symptoms.
It was edited by Smith CASE : A 52-year-old male with a past medical history of hypertension and COPD summoned EMS with complaints of chestpain, weakness and nausea. The diagnostic coronary angiogram identified only minimal coronary artery disease, but there was a severely calcified, ‘immobile’ aorticvalve.
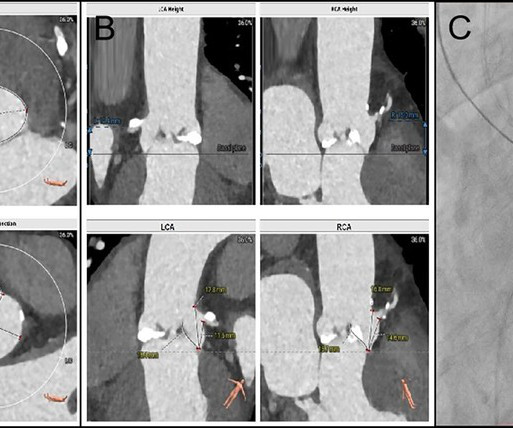
BackgroundFollowing transcatheter aorticvalve replacement, acute coronary obstruction is infrequent but potentially life-threatening, while delayed coronary obstruction is even more uncommon.Case summaryA 69-year-old male underwent TAVR and subsequently developed an acute obstruction in the left main coronary artery.
1, 2024 — Researchers at UTHealth Houston have identified genetic variants linked to a rare form of bicuspid aorticvalve disease that affects young adults and can lead to dangerous and potentially life-threatening aortic complications. tim.hodson Wed, 09/04/2024 - 15:53 Sept.
The Most Common Form of HVD One of the most prevalent and serious forms of heart valve disease is aortic stenosis (AS), a condition characterized by the narrowing of the aorticvalve opening, which affects approximately 5% of adults over 65a number expected to more than double by 2050.
About 276,000 patients have undergone a TAVR procedure in the United States. About 276,000 patients have undergone a TAVR procedure in the United States.
Aortic stenosis is a narrowing of the aorticvalve which prevents the aortic leaflets from opening and closing properly. Patients with aortic stenosis often have heart murmurs and experience debilitating symptoms including chestpain, dizziness, fatigue, shortness of breath and an irregular heartbeat.
Aortic stenosis is a narrowing of the aorticvalve which prevents the aortic leaflets from opening and closing properly. Patients with aortic stenosis often have heart murmurs and experience debilitating symptoms including chestpain, dizziness, fatigue, shortness of breath and an irregular heartbeat.
It showed reduced LV function — significant concentric LVH — a dilated left atrium — severe aortic stenosis ( seemingly in need of prompt valve replacement ) — and at least moderate pulmonary hypertension , with resultant moderate pulmonary regurgitation. The plan was to proceed as soon as possible with aorticvalve replacement.
Apparently he denied chestpain. JAMA 2000) showed that 1/3 of patients with STEMI, and 1/3 of patients with NSTEMI, present without chestpain. Chestpain and Concordant ST Depression in a patient with aorticvalve and previously normal angiogram Right Bundle Branch Block and ST Depression in V1-V3.
A 69 year old woman with a history of hypertension presented to the emergency department by EMS for evaluation of chestpain and shortness of breath. She awoke in the morning with sharp chestpain which worsened throughout the morning. As her pain worsened, so did her dyspnea. This was written by Hans Helseth.
Scenario 1 : The patient presents with 24 hours of substernal chestpain. Ninety percent of patients with reperfusion attained a maximum T wave negativity of 3 mm or more within 48 hours after the onset of chestpain in the lead that initially displayed the greatest ST segment elevation. Below is his presentation ECG.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.























Let's personalize your content