This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The study, called IVUS-DCB, is the first randomized controlled trial to demonstrate the clinical benefits of using IVUS in angioplasty procedures for peripheral artery disease (PAD), a condition in which plaque builds up in arteries in the legs. Half were randomly assigned to receive IVUS plus angiography and half received angiography alone.
PTA+DCB, P Key findings include: · One-year primary patency (freedom from both clinically driven target lesion revascularization and duplex ultrasound-derived restenosis) did not differ between groups, despite the significant difference in baseline calcification. · DA+DCB versus 5.9% versus 21.1%, P =0.014). 3 · One-year rates of TLR (16.6%
In this week’s View, Dr. Eagle looks at the difference between quantitative coronary angiography versus intervascular ultrasound to guide PCI. He then discusses paclitaxel-coated balloon catheters vs uncoated balloon angioplasty for treating coronary in-stent restenosis.
During the roundtable, participants highlighted the potential of IVUS in guiding revascularization procedures, such as angioplasty and stenting, to optimize outcomes for patients. They also emphasized the need for further research and evidence to support the integration of IVUS into routine clinical practice.
We aimed ultrasound-guided punctures in the proximal two-thirds of axillary arteries with diameters ≥2 mm to insert 7 cm/4 Fr short introducers. Overall, 27/36 procedures were interventional, including 6 aortic valvuloplasties, 6 balloon angioplasties, and 15 stenting procedures. We administrated intra-arterial verapamil (1.25 mg)
Bedside ultrasound with no apparent wall motion abnormalities, no pericardial effusion, no right heart strain. A comparison of electrocardiographic changes during reperfusion of acute myocardial infarction by thrombolysis or percutaneous transluminal coronary angioplasty. Aorta briefly viewed, appears normal caliber and diameter.
After guidewire crossing, balloon angioplasty was performed, and a drug-eluting stent was deployed. An intravascular ultrasound was also performed, which was negative for vessel dissection. The left circumflex had 80% proximal stenosis with minimal luminal irregularities in the mid to distal portion.
A lower extremity arterial ultrasound revealed elevated velocities in the right proximal superficial femoral artery. Based on these results, Dormu performed a percutaneous transluminal balloon angioplasty and a mechanical atherectomy and stenting of the right superficial femoral artery and stenting of the right superficial femoral artery.
His ED cardiac ultrasound (which is not at all ideal for detecting wall motion abnormalities, and is also very operator dependent for this finding) was significant for depressed global EF. The lesion was intervened on with balloon angioplasty and had subsequent TIMI 3 flow. The patient's initial troponin I was 2.0
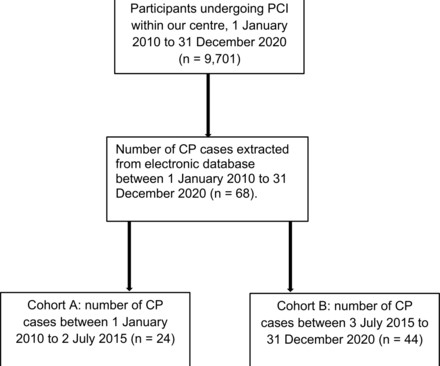
In cohort A, CP was most frequently caused by post-dilatation with non-compliant balloons (10 of 24 (42%); p=0.009); whereas in cohort B, common causes included guidewire exits (23 of 44 (52%)), followed by stent implantation (10 of 44 (23%)). Conclusion The incidence of CP is increasing as more complex PCI is performed.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content