This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
(MedPage Today) -- Submaximal balloon angioplasty for symptomatic intracranial atherosclerotic stenosis (ICAS) improved outcomes over aggressive medical management alone, the BASIS trial from China showed. The incidence of the composite of any.
Intracranial atherosclerotic stenosis is a leading cause of stroke with a significant risk of recurrent ischemic events despite aggressive medical management. However, 3 percutaneous angioplasty and stenting randomized trials showed negative or neutral results. Stroke, Volume 56, Issue 4 , Page e114-e118, April 1, 2025.
Is balloon angioplasty plus medical management superior to medical management alone in patients with symptomatic intracranial atherosclerotic stenosis?
The goal of the DCB-BIF trial was to assess the efficacy of drug-coated balloon (DCB) angioplasty of residual side branch stenosis in coronary bifurcation lesions treated with a provisional stenting strategy.
Introduction:Traditional endovascular treatment for acutely symptomatic intracranial atherosclerotic disease (ICAD) includes balloon angioplasty and stenting. Catheter mediated angioplasty (or “Dotter” angioplasty) has been previously described for extracranial carotid and peripheral arteries.
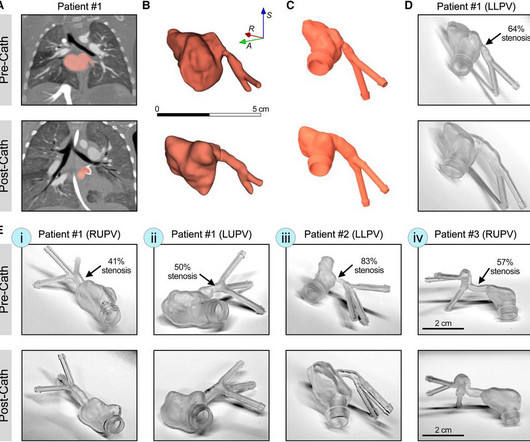
IntroductionPrimary pulmonary vein stenosis (PVS) is a rare congenital heart disease that proves to be a clinical challenge due to the rapidly progressive disease course and high rates of treatment complications.
IntroductionVertebral artery stenting represents a viable option in treating symptomatic vertebral artery atherosclerotic stenosis. We included articles reporting patients > 18 years old with symptomatic extracranial vertebral artery stenoses due to atherosclerosis treated with stenting (with or without angioplasty).
The objective of our study is to identify factors associated with SBIs following middle cerebral artery (MCA) stenting or balloon angioplasty.Methods:We retrospectively reviewed patients who underwent MCA stenting or balloon angioplasty, including those with symptomatic, atherosclerotic MCA stenosis of 50%. 14.74], p=0.012).
Asymptomatic high-grade carotid stenosis is an important therapeutic target for stroke prevention. Features like intraplaque hemorrhage on MRI and echolucency on B-mode ultrasonography can identify patients at higher risk of stroke with asymptomatic stenosis.
Sacharias von Kochpresented " Real-World Usage of Prevail Paclitaxel-Coated Balloon Compared with Other Contemporary Drug-Coated Balloons" This is atwo-year analysis from the Swedish Coronary Angiography and Angioplasty (SCAAR) Registry in more than 6,000 patients. This study is a pooled analysis from the U.S.
Baseline angiograms were reviewed to assess the presence or absence of intracranial stenosis lesions (IS+ Vs IS-) different than the target occlusion. Further research is warranted to explore the diagnostic value of multiple intracranial stenosis in patients undergoing mechanical thrombectomy. minutes; p=0.018). Vs 3; p=0.036).Conclusions:Our
Stroke, Volume 56, Issue Suppl_1 , Page ADP36-ADP36, February 1, 2025. All patients had headache, and funduscopic examination demonstrated papilledema for all patients. All patients had headache, and funduscopic examination demonstrated papilledema for all patients.
Trials included were: SYNTAX (TAXUS Drug-Eluting Stent Versus Coronary Artery Bypass Surgery for the Treatment of Narrowed Arteries), PRECOMBAT (Bypass Surgery Versus Angioplasty Using Sirolimus-Eluting Stent in Patients With Left Main Coronary Artery Disease), NOBLE (PCI vs. CABG in the Treatment of Unprotected Left Main Stenosis), and EXCEL [Evaluation (..)
Background:In stroke patients undergoing EVT, angioplasty and stenting (A&S) has been described as a bailout technique when thrombectomy fails or intracranial stenosis is suspected. Stroke, Volume 55, Issue Suppl_1 , Page AWMP88-AWMP88, February 1, 2024.
3% sodium alginate solution was cast into a stenosis mold and crosslinked in a 40% calcium chloride. After angioplasty (Gateway PTA Balloon Catheter 3.5x20mm, Boston Scientific) and stenting (Wingspan 2.5mmx15mm, Stryker) were performed the residual stenosis was <10% (Figure 1).
Background:Hemodynamic evaluation is crucial in assessing stroke risk in patients with symptomatic intracranial atherosclerotic stenosis (sICAS). Stroke, Volume 56, Issue Suppl_1 , Page AWP286-AWP286, February 1, 2025. before PTAS. before PTAS.
Subclavian venoplasty is commonly performed for subclavian vein stenosis in patients with long-term dialysis lines or fistulae. Such stenosis may also occur in patients with previously implanted intra-cardiac devices. Venoplasty was performed using peripheral angioplasty balloons after which the device was implanted.
Balloon angioplasty seems to be the widely preferred treatment of choice. The stenosis was treated with a stent. ABSTRACT Introduction Pulmonary vein (PV) restenosis develops with reported incidence rates of up to 50%. years later he presented with an in-stent restenosis that was successfully treated with a stent-in-stent strategy.
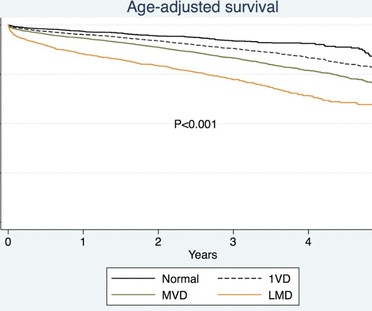
Data were collected from the Swedish Coronary Angiography and Angioplasty Registry and Swedish Web-system for Enhancement and Development of Evidence-based care in Heart disease Evaluated According to Recommended Therapies registries. Complications and mortality were higher in patients with LMD both during CA and PCI, HR 2.9 (1.1–7.6)
The aim of this study was to investigate outcomes in patients with left main disease with and without diabetes undergoing PCI versus CABG.METHODS:Individual patient data were pooled from 4 trials (SYNTAX [TAXUS Drug-Eluting Stent Versus Coronary Artery Bypass Surgery for the Treatment of Narrowed Arteries], PRECOMBAT [Bypass Surgery Versus Angioplasty (..)
Most neurointerventionalists (91%) diagnose ICAS‐LVO after a continued or recurrent occlusion or by the presence of fixed focal stenosis after multiple mechanical thrombectomy attempts. Most respondents (86%) preferred acute treatment of ICAS‐LVO with rescue stenting (RS)±angioplasty.
National Inpatient Sample (NIS) database from 2009 to 2020, evaluating patients who presented with stroke from ICAD and were treated with angioplasty and stenting and analyzed presenting co-morbidities and patient outcomes.
Recent research has identified venous sinus stenosis as a cause of IIH, a common treatment of which is venous stenting and angioplasty. An adverse event of this procedure is in‐stent stenosis (ISS), due to either neointimal hyperplasia or hypersensitivity to an element in the stent.
ml/h, P = 0.04), a higher likelihood of parent artery stenosis (65% vs. 20.8%, P < 0.001), and increased need for angioplasty or stenting (50% vs. 17%, P < 0.001). Follow-up lesion volumes and functional outcomes were similar; however, the mismatch group showed a slower infarct growth rate (3.8 ml/h vs. 7.5
A comparison of electrocardiographic changes during reperfusion of acute myocardial infarction by thrombolysis or percutaneous transluminal coronary angioplasty. Two ECG patterns were described by the original investigators in 1982 as being consistent with a Wellens’ Syndrome prediction of high-grade LAD stenosis. Am Heart J.
Introduction:An optimal strategy for the treatment of intracranial atherosclerotic disease (ICAD) has remained unclear, despite medical therapy (antiplatelet therapy and LDL control management) or endovascular therapy (angioplasty or stenting). 41.40) vs. MT: 9.15% (2.69-25.78), 25.78), P<0.0001 Mann-Whitney test).
Treatment of ICAS‐LVO with rescue stenting and/or angioplasty has shown promising outcomes, but diagnosing ICAS‐LVO during MT can be challenging [2, 3]. Most neurointerventionalists (91%) diagnose ICAS‐LVO after a continued or recurrent occlusion or by the presence of fixed focal stenosis (FFS) after multiple MT attempts.
Rescue treatment with stenting, balloon angioplasty, and/or intraarterial thrombolysis or antiplatelets are often required to treat the underlying stenosis. IntroductionIntracranial atherosclerotic disease (ICAD) is associated with up to 32% of posterior circulation strokes.1
Sacharias von Kochpresented " Real-World Usage of Prevail Paclitaxel-Coated Balloon Compared with Other Contemporary Drug-Coated Balloons" This is atwo-year analysis from the Swedish Coronary Angiography and Angioplasty (SCAAR) Registry in more than 6,000 patients. This study is a pooled analysis from the U.S.
Our findings suggest that targeting cellular mitochondrial respiration could be a novel therapeutic for patients with hypertension undergoing vascular angioplasty. A total of 36 202 cells from carotid arteries with or without balloon injury were included in single-cell RNA-sequencing analysis.
The left circumflex had 80% proximal stenosis with minimal luminal irregularities in the mid to distal portion. After guidewire crossing, balloon angioplasty was performed, and a drug-eluting stent was deployed. An intravascular ultrasound was also performed, which was negative for vessel dissection.
Options include initial angioplasty and/or stenting of the cervical lesion followed by intracranial thrombectomy versus Dotter navigation of catheters through the cervical lesion to first target the intracranial LVO. The degree of cervical ICA stenosis following thrombectomy improved from 96.5%
Angiogram --LAD is a large-caliber vessel that wraps around the apex --There is a tubular 80% in the ostial LAD that was relatively smooth but did not resolve with repeated doses of IC nitroglycerin --There is a tiny D1, medium D2, and small D3 Lesion on Prox LAD: Ostial 80% stenosis. Pre- procedure TIMI III flow was noted. Am Heart J.
LAD plaque with 0-25 percent stenosis. Given that the patient has had an abnormal elevated troponin, would suggest a Cardiology evaluation. --The LAD has moderate 40% ostial-proximal LAD stenosis and severe 90% mid LAD stenosis involving first diagonal branch. --The Now, with elevated troponins, Wellens' syndrome is likely.
Dormu performed an aortogram of the bilateral lower extremity with bilateral iliac runoff, which revealed a 90% stenosis of the right superficial femoral artery and 100% occlusion of all three tibial vessels. These studies revealed an 80% stenosis of the left superficial femoral artery and 100% occlusion of all three tibial vessels.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. Am Heart J (1989) 117 : pp 657-665. de Zwaan C., Wellens H.J.J., Am Heart J (1982) 103 : pp 730-736. Doevendans P.A., Gorgels A.P., van der Zee R.,
Patient underwent emergent mechanical thrombectomy with ADAPT to TICI3 revascularization with future plan for possible angioplasty and stenting of R vertebral stenosis. CT perfusion was without mismatch. Subsequently admitted to neurocritical care unit and treated with dual antiplatelet therapy.
61,62) The interventional community defines occlusive LM disease as >50% by FFR, or ≥75% stenosis,(63) but urgent or emergent intervention on lesions not meeting these thresholds is only imperative if it is a thrombotic lesion and the patient has refractory ischemic symptoms (i.e. Widimsky P et al. TIMI 0/1 flow).(61,62) Knotts et al.
Marked differences can be seen in the prevalence of coronary artery stenosis at autopsy by age and gender. In 30-39 year old women the rate of coronary stenosis at autopsy was 5/1,545 (0.3%) while 60-69 year old men had a prevalence of 12%, almost 40 times higher. The results of this dataset by age and gender follow.
Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. Wellens' original Papers : de Zwaan C, Bär FW, Wellens HJ. Am Heart J. 1982 Apr;103(4 Pt 2):730-6. de Zwaan C et al. Am Heart J. 2000 Mar;139(3):430-6.
Cath report later that afternoon, around 25 hours since arrival: "There was a 70% proximal LAD stenosis secondary to a spontaneous coronary dissection with narrowing of the proximal LAD to at least 50% stenosis. Severe hypokinesis of the anteroseptal, anterior, inferoseptal, and apical myocardium. Normal RV function.
Note that this obvious STEMI does not have 100% stenosis at the time of cath. Normal flow (TIMI-3) before mechanical reperfusion therapy is an independent determinant of survival in acute myocardial infarction: analysis from the primary angioplasty in myocardial infarction trials. Circulation. 2001;104:636–641.
Cath around 1730: Left main: normal LAD: prox LAD 30% stenosis immediately followed by a "99-100% thrombus filled occlusion" involving the proximal and mid LAD, as well as a large diagonal branch, with TIMI 1 flow pre-procedure. Cardiologist interpretation: "Technically does not meet STEMI criteria but concerning for ischemia."
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













































Let's personalize your content