This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Background Drug-eluting stents (DESs) have become the gold standard of coronary angioplasty since their inception in 2002. vs 57.5%, p=0.010), a greater average number of stents implanted per patient (1.72±0.92 vs 57.5%, p=0.010), a greater average number of stents implanted per patient (1.72±0.92
milla1cf Wed, 03/13/2024 - 16:52 March 13, 2024 — In the largest randomized clinical trial and first of its kind to date in the United States, a team led by investigators at Beth Israel Deaconess Medical Center (BIDMC) assessed the efficacy and safety of using a drug-coated balloon in patients undergoing coronary angioplasty.
Among the patients included, those with diabetes exhibited higher rates of adverse events, including death, spontaneous myocardialinfarction (MI), and repeat revascularization. Pooled data from four trials were analyzed, encompassing patients undergoing PCI or CABG for left main disease.
The United States has been way behind other nations in using drug-coated balloons (DCB) to treat coronary in-stent restenosis (ISR), but that’s about to change thanks to the FDA approval of Boston Scientific’s AGENT Drug-Coated Balloon. vs. 24.0%) Target vessel myocardialinfarction (6.4% vs 12.3%) Stent thrombosis (0.0%
Patients with diabetes experienced higher rates of 5-year death (158/1104 [Kaplan-Meier rate, 14.7%] versus 297/3289 [9.3%];P<0.001), spontaneous myocardialinfarction (MI; 67/1104 [6.7%] versus 114/3289 [3.7%];P<0.001), and repeat revascularization (189/1104 [18.5%] versus 410/3289 [13.2%];P<0.001).
A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. Am Heart J. 2000;139:430–436. Am J Cardiol.
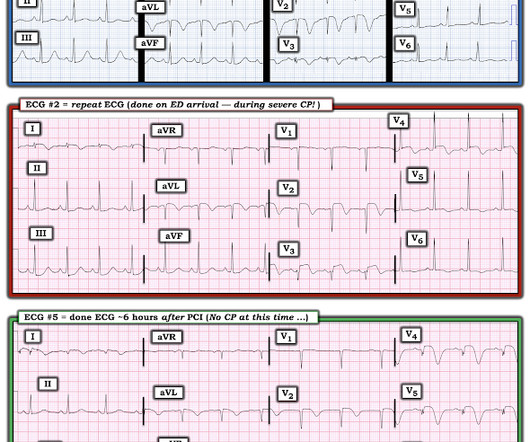
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. Clin Cardiol 2022 4. Herman, Meyers, Smith et al. Eur Heart J Digital Health 2024 5. McLaren and Smith.
A stent was placed. In my experience, all Wellens' with significant myocardialinfarction have evolution from type A waves to type B waves over 6-24 hours' time , so that the presence of type A or type B waves, I believe, are simply a matter of the timing of recording and the rapidity of evolution. de Zwaan C., Wellens H.J.J.,
An open 90% LAD was stented. Here is the ECG the next AM: There was so little infarction that there are lateral, but no anterior reperfusion T-waves (normally, there would be Wellens' type waves after LAD reperfusion). Here is some older but very interesting literature on TIMI myocardial perfusion grade and ST resolution : 1.
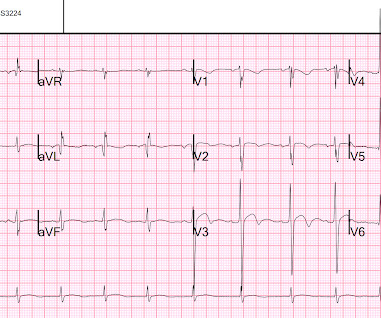
A male in late middle age with a history of RCA stent 8 years prior complained of chest pain. See this article by Widimsky: Primary angioplasty in acute myocardialinfarction with right bundle branch block: should new onset right bundle branch block be added to future guidelines as an indication for reperfusion therapy [link]
The OM-1 was opened and stented, then the LAD was stented 3 days later. The acute infarct-related artery was off the circumflex and the affected wall was posterior (STEMI). The LAD had a 75% proximal lesion that by fractional flow reserve was hemodynamically significant. The posterior leads were falsely negative.
At the bottom of the post, I have re-printed the section on aVR in my article on the ECG in ACS from the Canadian Journal of Cardiology: New Insights Into the Use of the 12-Lead Electrocardiogram for Diagnosing Acute MyocardialInfarction in the Emergency Department Case 1. Widimsky P et al. O'Gara PT, Kushner FG, Ascheim DD, et al.
Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardialinfarction. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. Am Heart J. Am Heart J.
It was opened and stented. The Cath lab was activated. Repeat ECG while waiting for cath team, t = 56 min after arrival: It is getting worse Angiogram showed 99% acute proximal LAD thrombosis. Peak trop > 50,000 ng/L Formal Bubble contrast echo Severe LV systolic dysfunction.
Successful primary angioplasty of the mid-circumflex artery towards the main marginal branch with the implantation of a drug-eluting stent. Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardialinfarction patients. Good angiographic result.
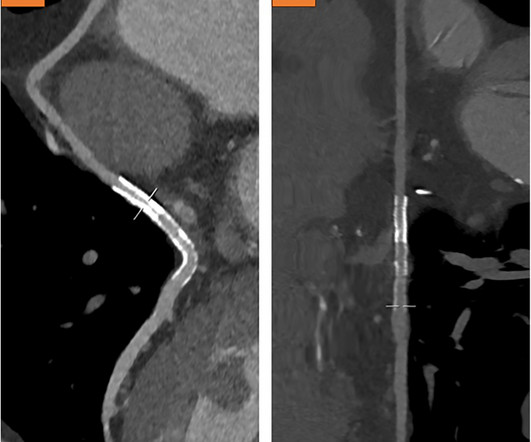
The lesion was intervened on with balloon angioplasty and had subsequent TIMI 3 flow. It was thought to be an in stent restenosis and thrombosis from a DES placed in the same region 6 months prior. There was initially TIMI 0 flow. His troponin I peaked at 97 ng/mL (very large MI!). What can we learn?
ng/mL This single initial troponin at this level, in the context of chest pain, is high enough to be diagnostic of acute myocardialinfarction. INTERVENTION * Successful angioplasty and stenting (drug eluting) of the mid LAD * Successful angioplasty of the ostial 1st diagonal Learning points: 1.
In their haste to hyperventilate about MINOCA, the authors don’t highlight the high percentage of cardiac interventions that are needed in patients with conventional, common epicardial disease - 80% need a coronary stent and 10% need open heart surgery. Women also had more cardiovascular risk factors, including hypertension (66.6%
When one of these arteries becomes completely blocked by a blood clot, it results in a heart attack, also known as MI (Myocardialinfarction). When a person experiences a heart attack or myocardialinfarction, they may feel chest pain and other symptoms in different parts of their body.
Initial diagnostics indicated non-ST-elevation myocardialinfarction, leading to immediate intervention. A combination of balloon angioplasty, stent implantation, and intra-arterial thrombolysis with recombinant tissue plasminogen activator (rt-PA) was employed, resulting in significant thrombus reduction and improved coronary flow.
A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. A stent was placed.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content