This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. Am Heart J. 2000;139:430–436. Am J Cardiol.
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
Objective Coronary angiography (CA) and percutaneous coronary intervention (PCI) is of great importance during non-ST-segment elevation myocardialinfarction (NSTEMI) management. Conclusion Coronary lesions (>50% stenosis) are strong predictors of mortality in elderly patients with NSTEMI. –7.6) and HR 4.5 (1.6–12.5).
Timing of revascularization in patients with transient ST segment elevation myocardialinfarction: a randomized clinical trial. A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty. Lemkes et al. Am Heart J.
In my experience, all Wellens' with significant myocardialinfarction have evolution from type A waves to type B waves over 6-24 hours' time , so that the presence of type A or type B waves, I believe, are simply a matter of the timing of recording and the rapidity of evolution. Am Heart J (1989) 117 : pp 657-665. de Zwaan C.,
ng/mL This single initial troponin at this level, in the context of chest pain, is high enough to be diagnostic of acute myocardialinfarction. LAD plaque with 0-25 percent stenosis. If trops are negative and there is <50% stenosis, then the patient is safe for discharge, even if the HEART score or EDACS score are elevated.
Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardialinfarction. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. Am Heart J.
Read our recent editorial: Hyperacute T-waves Can Be a Useful Sign of Occlusion MyocardialInfarction if Appropriately Defined. Note that this obvious STEMI does not have 100% stenosis at the time of cath. It showed a mid LAD culprit with 95% with no pre intervention timi flow listed. Pol Arch Intern Med. 2017;127:401–411.
Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardialinfarction patients. In the setting of evolving infarction — development of AIVR often heralds the onset of reperfusion ( following thrombolysis, acute angioplasty, or spontaneous reperfusion ).
Cath around 1730: Left main: normal LAD: prox LAD 30% stenosis immediately followed by a "99-100% thrombus filled occlusion" involving the proximal and mid LAD, as well as a large diagonal branch, with TIMI 1 flow pre-procedure. Next trop 85,528 ng/L (consistent with a massive myocardialinfarction), none further measured.
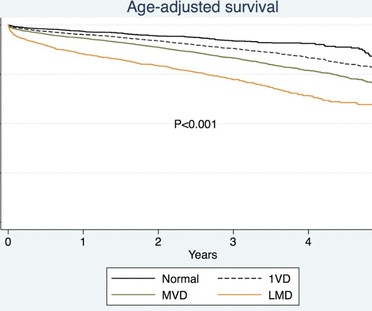
Among the patients included, those with diabetes exhibited higher rates of adverse events, including death, spontaneous myocardialinfarction (MI), and repeat revascularization. Patients were stratified based on diabetes status, and various outcome measures were assessed using Kaplan-Meier event rates and Cox model hazard ratios.
Patients with diabetes experienced higher rates of 5-year death (158/1104 [Kaplan-Meier rate, 14.7%] versus 297/3289 [9.3%];P<0.001), spontaneous myocardialinfarction (MI; 67/1104 [6.7%] versus 114/3289 [3.7%];P<0.001), and repeat revascularization (189/1104 [18.5%] versus 410/3289 [13.2%];P<0.001).
At the bottom of the post, I have re-printed the section on aVR in my article on the ECG in ACS from the Canadian Journal of Cardiology: New Insights Into the Use of the 12-Lead Electrocardiogram for Diagnosing Acute MyocardialInfarction in the Emergency Department Case 1. Widimsky P et al. TIMI 0/1 flow).(61,62) Knotts et al.
Marked differences can be seen in the prevalence of coronary artery stenosis at autopsy by age and gender. In 30-39 year old women the rate of coronary stenosis at autopsy was 5/1,545 (0.3%) while 60-69 year old men had a prevalence of 12%, almost 40 times higher. The results of this dataset by age and gender follow.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content