This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
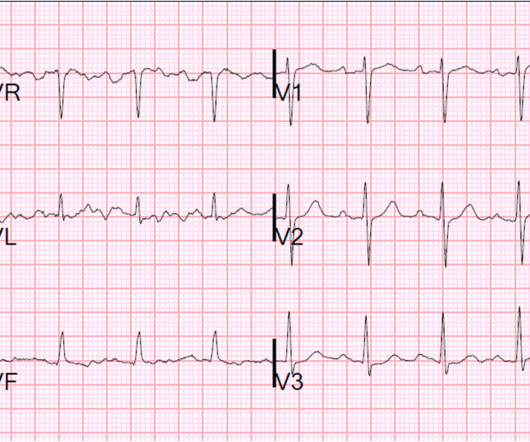
He had an immediate ED ECG: There is artifact, but the findings appear to be largely gone now The diagnosis is acute MI, but not STEMI. There is about 1 mm of STE in aVR I con sidered but rejected subendocardial ischemia. Is it subendocardial ischemia, or inferior MI? Here is his prehospital ECG: Diagnosis?
Echo on the day after admission showed EF of 30-35% and antero-apical wall akinesis with an LV thrombus [these frequently form in complete or near complete (no early reperfusion) anterior STEMI because of akinesis/stasis] 2 more days later, this was recorded: ST elevation is still present. The LAD has reperfused early. This was recorded 2.5
Precordial ST depression may be subendocardial ischemia or posterior STEMI. If you thought it might be a posterior STEMI, then you might have ordered a posterior ECG [change leads V4-V6 around to the back (V7-V9)]. I have warned in the past that one must think of other etiologies of ischemia when there is tachycardia.
Computer read: "Non-specific ST abnormality, consider anterior subendocardial ischemia" There are very poor R-waves in V1-V4 suggesting old anterior MI. Firstly, subendocardial ischemia does not localize on 12-Lead ECG. But the real question at hand is: Are these precordial ST-depressions a result of subendocardial ischemia?
For example — We would not normally expect to see more ST elevation after PCI ( as we do in ECG #3 ) — unless reperfusion of the "culprit" artery with the procedure was not successful — or — unless additional ECGs done prior to PCI showed additional ST elevation occurred before angioplasty opened the occluded vessel.
Here is the prehospital ECG, with pain: Hyperacute anterolateral STEMI The medics had activated the cath lab and the patient went for angiogram and had a 95% stenotic LAD with TIMI-3 flow. For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. Type B waves are deeper and symmetric.
Inferior ST Depression does NOT mean there is inferior subendocardial ischemia; it is generally reciprocal to high lateral (aVL) subepicardial ischemia (OMI/STEMI) == MY Comment by K EN G RAUER, MD ( 2/10/2023 ): == There are certain patterns in ECG interpretation that experienced providers are able to immediately recognize.
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? Physician interpretation: "No STEMI." Physician: "No STEMI." Cardiologist interpretation: "Technically does not meet STEMI criteria but concerning for ischemia."
This strongly suggests reperfusing RCA ischemia. Troponins, echocardiogram An echocardiogram showed inferobasilar hypokinesis, further supporting a diagnosis of regional ischemia , likely of the area supplied by the RCA. A recent study found that SCAD causes almost 20% of STEMI in young women. There is also a Q-wave in III.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
The ECG is diagnostic of LAD occlusion (or even left main occlusion possibly), with the classic pattern of RBBB and LAFB with huge concordant STE in V1-V2, I, and aVL, with reciprocal depression in most other leads (and/or a component of subendocardial ischemia pattern). Code STEMI was activated. This is "shark fin" morphology.
Normally, concavity in ST segments suggests absence of anterior ischemia (though concavity by itself is not reassuring - see this study ). The lesion was intervened on with balloon angioplasty and had subsequent TIMI 3 flow. In there ECG evidence of possible ongoing ischemia? (ie, There was initially TIMI 0 flow.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content