This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion. Am Heart J.
A male in late middle age with a history of RCA stent 8 years prior complained of chestpain. EMS recorded the following ECG: What do you see? The computer read "Right Bundle Branch Block" There is RBBB and LAFB, which can make it difficult to see the end of the QRS.
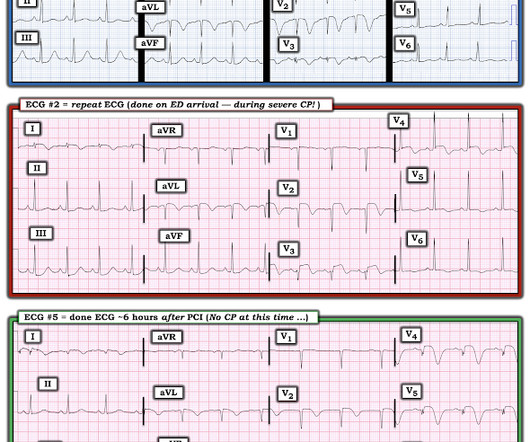
A 40-something woman called 911 in the middle of the night for Chestpain that was intermittent. On arrival, she complained of severe pain. The medics had recorded this ECG and were uncertain whether it was recorded during chestpain: Let's get a better image with use of the PM Cardio app : What do you think?
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. Case A 40-something male presented to triage. There are classic Wellens' waves in V2-V5. Am Heart J.
Introduction:Subacute stent thrombosis (ST) is related to high rates of cardiac reinfarction. The patient’s chestpain (CP) was not alleviated with initial revascularization of his left circumflex (LCx) ST, requiring PCI to his right coronary artery (RCA) chronic total occlusion (CTO). We present a case of reinfarction from ST.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. The patient was transferred to CCU to consider surgical options.
This male in his 40's had been having intermittent chestpain for one week. He awoke from sleep with crushing central chestpain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. A stent was placed. Type B waves are deeper and symmetric. Wehrens X.H.,
This means that at every age, the probability a man complaining of chestpain has significant underlying coronary disease as a cause of this chestpain is much higher than a woman complaining of chestpain. Thanks for reading Dr. The data is overwhelming every way you can possibly look at it.
This 42 yo diabetic male presented with cough and foot pain. In spite of aggressive questioning, he denied chestpain, but he did tell one triage nurse that he had had some chest burning, and so he underwent an ECG: There are deep Q-waves and QS-waves in precordial leads V2-V3, with a bit of R-wave left in V4.
He reported typical chestpain since 4H AM and arrived at our ED at 10h with ongoing chestpain. Successful primary angioplasty of the mid-circumflex artery towards the main marginal branch with the implantation of a drug-eluting stent. You must record frequent serial ECGs for patients with chestpain.
As of now CT angiograms cannot replace conventional coronary angiography while planning procedures like balloon angioplasty. Balloon angioplasty is removal of blocks from the blood vessels using slender long tubes with high pressure balloons at the tip. CT coronary angiogram can be done as an outpatient test, in the X-ray department.
This can block smooth flow of blood and the person can develop chestpain. When medications and/or procedures like balloon angioplasty are unable to re-establish good blood flow to the heart, these blood vessels can be bypassed by an operation known as coronary artery bypass grafting or CABG.
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chestpain and SOB. She had one episode of pain the previous night and two additional episodes early on morning the morning she presented. Deep breaths are painful and symptoms come and go.
However, seeking immediate medical help is crucial if you experience chestpain, shortness of breath or dizziness. Procedures such as angioplasty, stenting and bypass surgery can restore blood flow to the heart and improve function.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chestpain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
While men often report crushing chestpain as the most prominent symptom, women might experience subtler symptoms like shortness of breath, nausea, or back pain. Women might describe it as a tightness, pressure, or squeezing sensation rather than a sharp pain.
No chestpain. His inpatient clinicians did not think that an urgent angiogram was warranted given that he was chestpain free, his EKG appeared nondiagnostic, and serial troponins were not elevating beyond 2 ug/L. The lesion was intervened on with balloon angioplasty and had subsequent TIMI 3 flow. Why is this?
His comments/questions are inserted below the ECG: A 50-something woman presented with 3 days of intermittent chestpain that became worse on the day of presentation, with diaphoresis and radiation to the left arm, as well as abdominal pain. Everolimus-Eluting Stents or Bypass Surgery for Left Main Coronary Artery Disease.
When a person experiences a heart attack or myocardial infarction, they may feel chestpain and other symptoms in different parts of their body. Although both techniques have advantages and limitations, primary angioplasty is the chosen therapy in most cases. So, how do you recognize a heart attack?
A 30 year old African American Male presented to the ED with chestpain that occurred the day before. There was no pain on the day of presentation. 2019.06.007) (Full text here: [link] ) The ECG above is diagnostic of Wellens' syndrome (full reference below): 1) Episode of anginal chestpain that is resolved (GONE!)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content