This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. What do you think the prehospital ECG showed (with pain)?
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the Emergency Department with severe intermittent chestpain. He denied any lightheadedness, shortness of breath, vomiting, or abdominal pain. Barely any STE, and thus not meeting STEMI criteria.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion.
A 70-year-old man calls 911 after experiencing sudden, severe chestpain. The precordial ST-depression pattern on this ECG (and in this clinical setting) should immediately raise suspicion of Posterior STEMI! But if there is none - then you are looking at least at an Isolated Posterior STEMI until proven otherwise.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." examined SCAD presenting as STEMI (unlike Hassan et al.
There is clearly sufficient STE for STEMI criteria in leads V2 and aVL, but lead I has less than 1.0 mm of STE - thus, technically this ECG does not meet STEMI criteria, although it is a quite obvious OMI. This ECG was immediatel y discussed with the on-call cardiologist who said the ECG was "concerning but not a STEMI."
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. So you are going to get to see what the ECG would have shown had you recorded one during pain! Am Heart J.
Echo on the day after admission showed EF of 30-35% and antero-apical wall akinesis with an LV thrombus [these frequently form in complete or near complete (no early reperfusion) anterior STEMI because of akinesis/stasis] 2 more days later, this was recorded: ST elevation is still present. He had been awakened by cough at 3 AM 2 days earlier.
A male in his 60's called 911 for chestpain. His pain was intermittent and he was vague about when it was present and when it was resolved. He had an immediate ED ECG: There is artifact, but the findings appear to be largely gone now The diagnosis is acute MI, but not STEMI. Here is his prehospital ECG: Diagnosis?
He reports significant chestpain at the base of his scapula on the right side along with new shortness of breath. Smith : there is some minimal ST elevation in V2-V6, but does not meet STEMI criteria. Transient STEMI has been studied and many of these patients will re-occlude in the middle of the night. Is it normal STE?
This was my thought: if this patient presented to the ED with chestpain, then this is an LAD occlusion. His ECG was repeated at this point: This shows a well developed anterior STEMI. To not see these findings is very common, and this patient would be given the diagnosis of NonSTEMI, with subsequent development of STEMI.
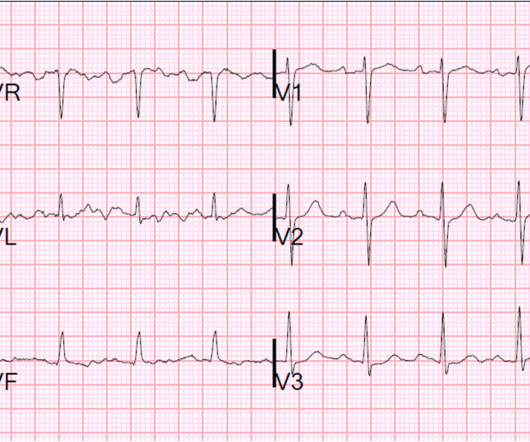
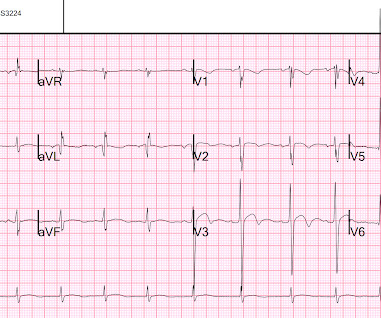
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chestpain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
NOTE: It's important to correlate ongoing circumstances at the time that a prior tracing was done ( ie, Was the patient stable and asymptomatic — or were they having chestpain, an exacerbation of heart failure, or some other ongoing process at the time the prior ECG was recorded? ).
This male in his 40's had been having intermittent chestpain for one week. He awoke from sleep with crushing central chestpain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. Type B waves are deeper and symmetric. Wehrens X.H., Doevendans P.A., Ophuis T.J.,
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chestpain and SOB. She had one episode of pain the previous night and two additional episodes early on morning the morning she presented. Deep breaths are painful and symptoms come and go.
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chestpain)? Here is the clinical informaton on ECG 2: A man in his 50s presented to the Emergency Department with acute chestpain that started within the past few hours.
Inferior ST Depression does NOT mean there is inferior subendocardial ischemia; it is generally reciprocal to high lateral (aVL) subepicardial ischemia (OMI/STEMI) == MY Comment by K EN G RAUER, MD ( 2/10/2023 ): == There are certain patterns in ECG interpretation that experienced providers are able to immediately recognize.
Written by Jesse McLaren A 75 year old with a history of CABG called EMS after 24 hours of chestpain. The patient has a history of CABG so some of these changes could be old, but with ongoing chestpain and bradycardia in a high risk patient this is still acute OMI until proven otherwise. HR 40, BP 135/70, RR16, O2 100%.
A male in late middle age with a history of RCA stent 8 years prior complained of chestpain. Here are three more dramatic cases that illustrate RBBB + LAFB Case 1 of cardiac arrest with unrecognized STEMI, died. EMS recorded the following ECG: What do you see?
He reported typical chestpain since 4H AM and arrived at our ED at 10h with ongoing chestpain. Unfortunately, the cardiologist waited until the next day to refer the patient for angiography and intervention because patient did not meet criteria for "STEMI"." The first ECG (10h14) showed TWI in inferior leads."
No chestpain. His inpatient clinicians did not think that an urgent angiogram was warranted given that he was chestpain free, his EKG appeared nondiagnostic, and serial troponins were not elevating beyond 2 ug/L. The lesion was intervened on with balloon angioplasty and had subsequent TIMI 3 flow. Why is this?
Code STEMI was activated. What is the Diagnosis in this 70-something with ChestPain? 68 minutes with chest compressions, full recovery. A man in his 80s with chestpain What, besides large anterior STEMI, is so ominous about this ECG? The patient arrived to the ED in cardiogenic shock but awake.
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
A 30 year old African American Male presented to the ED with chestpain that occurred the day before. There was no pain on the day of presentation. 2019.06.007) (Full text here: [link] ) The ECG above is diagnostic of Wellens' syndrome (full reference below): 1) Episode of anginal chestpain that is resolved (GONE!)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content