This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion. Am Heart J.
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the Emergency Department with severe intermittent chestpain. He denied any lightheadedness, shortness of breath, vomiting, or abdominal pain. TIMI flow alone cannot be used as an outcome definition for OMI or STEMI. =
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." This case occurred 10+ years ago. Lobo et al.
A 70-year-old man calls 911 after experiencing sudden, severe chestpain. New electrocardiographic criteria for posterior wall myocardial ischemia validated by percutaneous transluminal coronary angioplasty model of acute myocardial infarction. This case comes from Sam Ghali ( @EM_RESUS ). Thanks, Sam! Neth Heart J.
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. More outcome Peak troponin I was 0.58 Case A 40-something male presented to triage. Am Heart J.
There is a patient with persistent chestpain and an initial troponin I over 52 ng/L; 52 ng/L has an approximate 70% PPV for acute type I MI in a chestpain patient. Pain was severe and persistent. CT angiography chest assessing for PE and dissection negative. Heparin drip was initiated. Is there STEMI?
This causes angina, a type of chestpain which is characterized as refractory angina when this pain cannot be controlled by a combination of optimal medical therapy, angioplasty or bypass surgery, and is estimated to impact 600,000 to 1.8 million patients in the United States.
There was a good outcome. We believe this represents a form of “toxicomythology” given the millions of doses of beta -blockers administered in the past to patients with hyperadrenergic states, and a paucity of evidence of adverse outcomes (12). This would treat both SVT or sinus tachycardia. Later, he was found to have used cocaine.
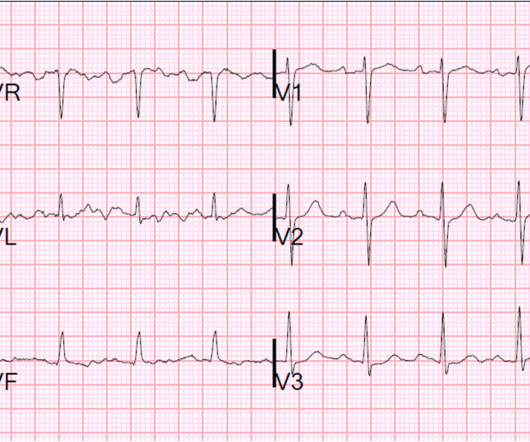
This male in his 40's had been having intermittent chestpain for one week. He awoke from sleep with crushing central chestpain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. Type B waves are deeper and symmetric. Wellen's syndrome is a Reperfusion syndrome.
This year’s theme, “Advancing Cardiovascular Care for All” brings the latest practice-changing breakthroughs, along with top experts debating and discussing outcomes of highly-anticipated clinical trials. 24 from April 6 - 8, 2024 in Atlanta, GA at the Georgia World Congress Center.
This 42 yo diabetic male presented with cough and foot pain. In spite of aggressive questioning, he denied chestpain, but he did tell one triage nurse that he had had some chest burning, and so he underwent an ECG: There are deep Q-waves and QS-waves in precordial leads V2-V3, with a bit of R-wave left in V4.
This was my thought: if this patient presented to the ED with chestpain, then this is an LAD occlusion. These patients have worse outcomes: higher mortality, more CHF, higher biomarkers, and worse ejection fractions than the NonSTEMI patients with open arteries. This patient had continued and ongoing pain. Marti D et al.
Full case details and outcomes are below. The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chestpain)? Repeat 0157 with ongoing chestpain: Basically the same features diagnostic of LAD occlusion. Physician: "No STEMI."
A male in his 60's called 911 for chestpain. His pain was intermittent and he was vague about when it was present and when it was resolved. Outcome : Was it RCA or LCX with inferior MI? The RCA was opened with POBA ("plain old balloon angioplasty") and eptifibatide was started.
Signs include: Sudden loss of consciousness No pulse or breathing Collapse without prior chestpain or discomfort If someone experiences sudden cardiac arrest, it is crucial to begin CPR immediately and call the local emergency number. Without prompt treatment, parts of the heart muscle may become damaged or die.
A male in late middle age with a history of RCA stent 8 years prior complained of chestpain. It is highly associated with proximal LAD occlusion and bad outcomes. EMS recorded the following ECG: What do you see? I have annotated it here: The lines mark the end of the QRS and beginning of the ST segment.
Soviet biologist Trofim Lysenko famously rejected the objective reality of Mendelian genetics because it clashed with the Marxist philosophy that the environment, not genetics, was the primary determinant of outcomes. Atypical angina is classified as having any two of the three symptoms, and non-anginal pain any one of the three symptoms.
While men often report crushing chestpain as the most prominent symptom, women might experience subtler symptoms like shortness of breath, nausea, or back pain. Women might describe it as a tightness, pressure, or squeezing sensation rather than a sharp pain.
However, seeking immediate medical help is crucial if you experience chestpain, shortness of breath or dizziness. Early intervention can significantly improve outcomes and reduce the risk of complications. Procedures such as angioplasty, stenting and bypass surgery can restore blood flow to the heart and improve function.
His comments/questions are inserted below the ECG: A 50-something woman presented with 3 days of intermittent chestpain that became worse on the day of presentation, with diaphoresis and radiation to the left arm, as well as abdominal pain. This is her ECG: An obvious STEMI, but which artery? Widimsky P et al.
When a person experiences a heart attack or myocardial infarction, they may feel chestpain and other symptoms in different parts of their body. It is imperative to act swiftly when faced with such a medical emergency to ensure the best possible outcome. So, how do you recognize a heart attack?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


























Let's personalize your content