This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion. Am Heart J.
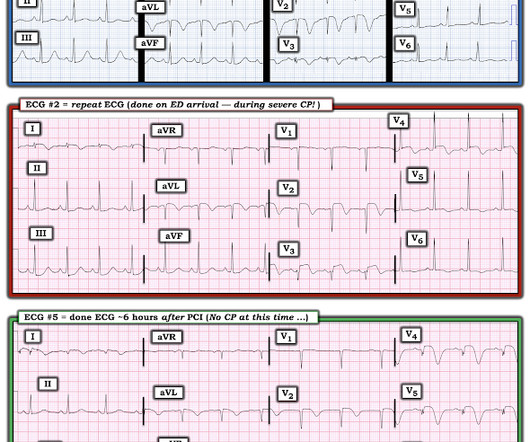
A 40-something woman called 911 in the middle of the night for Chestpain that was intermittent. On arrival, she complained of severe pain. The medics had recorded this ECG and were uncertain whether it was recorded during chestpain: Let's get a better image with use of the PM Cardio app : What do you think?
Sent by anonymous, written by Pendell Meyers A man in his 50s with no prior known medical history presented to the Emergency Department with severe intermittent chestpain. He denied any lightheadedness, shortness of breath, vomiting, or abdominal pain. Isn't it amazing?? Pol Arch Intern Med. 2017;127:401–411. Am J Cardiol.
A 70-year-old man calls 911 after experiencing sudden, severe chestpain. Electrocardiographic Manifestations: Acute posterior wall myocardialinfarction. Posterior myocardialinfarction: the dark side of the moon. This case comes from Sam Ghali ( @EM_RESUS ). Thanks, Sam! J Emerg Med 2001; 20:391-401.
[link] A 30 year-old woman was brought to the ED with chestpain. She had given birth a week ago, and she had similar chestpain during her labor. She attributed the chestpain to anxiety and stress, saying "I'm just an anxious person." This case occurred 10+ years ago. References Lobo AS et al.
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction.
He reports significant chestpain at the base of his scapula on the right side along with new shortness of breath. Timing of revascularization in patients with transient ST segment elevation myocardialinfarction: a randomized clinical trial. See these casese (and I have many others): First ED ECG is Wellens' (pain free).
There is a patient with persistent chestpain and an initial troponin I over 52 ng/L; 52 ng/L has an approximate 70% PPV for acute type I MI in a chestpain patient. Immediate and early percutaneous coronary intervention in very high-risk and high-risk non-ST segment elevation myocardialinfarction patients.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. The patient was transferred to CCU to consider surgical options. Clin Cardiol 2022 4. Herman, Meyers, Smith et al.
This male in his 40's had been having intermittent chestpain for one week. He awoke from sleep with crushing central chestpain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. Type B waves are deeper and symmetric. Am Heart J (1989) 117 : pp 657-665. de Zwaan C.,
ET Main Tent (Hall B1) - A Double-blind, Randomized Placebo Procedure-controlled Trial of an Interatrial Shunt in Patients with HFrEF and HFpEF: Principal Results From the RELIEVE-HF Trial - Empagliflozin After Acute MyocardialInfarction: Results of the EMPACT-MI Trial - CSL112 (Apolipoprotein A-I) Infusions and Cardiovascular Outcomes in Patients (..)
This 42 yo diabetic male presented with cough and foot pain. In spite of aggressive questioning, he denied chestpain, but he did tell one triage nurse that he had had some chest burning, and so he underwent an ECG: There are deep Q-waves and QS-waves in precordial leads V2-V3, with a bit of R-wave left in V4.
Marcus, G. Harvard Medical School, Boston, Massachusetts, USA. Metoprolol and atenolol are overwhelmingly beta-1 cardioselective. Beta-1 blockade decreases inotropy and chronotropy and has no vasoconstrictive effects. Only beta-2 blockade (e.g., Henry Ford Hospital. Henry Ford Hospital.
This was my thought: if this patient presented to the ED with chestpain, then this is an LAD occlusion. Usefulness of automated serial 12-lead ECG monitoring during the initial emergency department evaluation of patients with chestpain. Ann Emerg Med 1998;31(1):3-11. Wang T, Zhang M, Fu Y, et al. Marti D et al.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chestpain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chestpain and SOB. She had one episode of pain the previous night and two additional episodes early on morning the morning she presented. Deep breaths are painful and symptoms come and go.
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chestpain)? Here is the clinical informaton on ECG 2: A man in his 50s presented to the Emergency Department with acute chestpain that started within the past few hours.
Written by Jesse McLaren A 75 year old with a history of CABG called EMS after 24 hours of chestpain. The patient has a history of CABG so some of these changes could be old, but with ongoing chestpain and bradycardia in a high risk patient this is still acute OMI until proven otherwise. HR 40, BP 135/70, RR16, O2 100%.
A heart attack, or myocardialinfarction, happens when an artery becomes blocked, reducing blood flow to the heart muscle. Understanding the difference between heart attack and cardiac arrest can help in recognizing symptoms, seeking prompt medical care, and even saving lives. What is a Heart Attack?
A male in late middle age with a history of RCA stent 8 years prior complained of chestpain. See this article by Widimsky: Primary angioplasty in acute myocardialinfarction with right bundle branch block: should new onset right bundle branch block be added to future guidelines as an indication for reperfusion therapy [link]
He reported typical chestpain since 4H AM and arrived at our ED at 10h with ongoing chestpain. Successful primary angioplasty of the mid-circumflex artery towards the main marginal branch with the implantation of a drug-eluting stent. You must record frequent serial ECGs for patients with chestpain.
No chestpain. His inpatient clinicians did not think that an urgent angiogram was warranted given that he was chestpain free, his EKG appeared nondiagnostic, and serial troponins were not elevating beyond 2 ug/L. The lesion was intervened on with balloon angioplasty and had subsequent TIMI 3 flow. Why is this?
At the bottom of the post, I have re-printed the section on aVR in my article on the ECG in ACS from the Canadian Journal of Cardiology: New Insights Into the Use of the 12-Lead Electrocardiogram for Diagnosing Acute MyocardialInfarction in the Emergency Department Case 1. Widimsky P et al. O'Gara PT, Kushner FG, Ascheim DD, et al.
This means that at every age, the probability a man complaining of chestpain has significant underlying coronary disease as a cause of this chestpain is much higher than a woman complaining of chestpain. Thanks for reading Dr. The data is overwhelming every way you can possibly look at it.
Other cases of LAD OMI with RBBB/LAFB: A man in his 40s who really needs you to understand his ECG Cardiac Arrest at the airport, with an easy but important ECG for everyone to recognize A woman in her 60s with 6 hours of chestpain, dyspnea, tachycardia, and hypoxemia Ventricular Fibrillation, ROSC after perfusion restored by ECMO, then ECG.
When one of these arteries becomes completely blocked by a blood clot, it results in a heart attack, also known as MI (Myocardialinfarction). When a person experiences a heart attack or myocardialinfarction, they may feel chestpain and other symptoms in different parts of their body.
A 30 year old African American Male presented to the ED with chestpain that occurred the day before. There was no pain on the day of presentation. 2019.06.007) (Full text here: [link] ) The ECG above is diagnostic of Wellens' syndrome (full reference below): 1) Episode of anginal chestpain that is resolved (GONE!)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
































Let's personalize your content