This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In addition, the criteria require the absence of precordial Q waves, the presence of history of angina, and normal or slightly elevated cardiac serum markers. How common is thrombosis in the culprit artery of Wellen syndrome ? However by no means, we can say thrombosis do not occur. Wellens is a glorified subset of ACS.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction.
Given the consistency of the clinical profile with typical angina, associated risk factors, and abnormal ECG findings, a cardiology consult was promptly requested. Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. Severe Hypoxia b.
As hours go by, these T inversions always evolve , [unless 1) there is re-occlusion, in which case they go upright and become hyperacute, with or without additional ST elevation, ("pseudonormalize") or 2) no infarction at all (negative troponin, true unstable angina with dynamic T-waves, in which they may normalize). Gottlieb SO, et al.
5 We are aware that the current consensus is that the propensity for plaques to rupture is independent of plaque size; however, in our opinion, the hypothesis that small atherosclerotic plaques are the most likely to rupture, with resulting occlusive thrombosis, is unproven. These are typical findings at sites of plaque rupture.
After percutaneous coronary intervention, DAPT was given for 1 month to patients presenting with stable angina. The primary end point was a composite of cardiac death, myocardial infarction, or stent thrombosis up to 1 year (Academic Research Consortium definite and probable). presented with acute coronary syndrome; 33.7%
At the time of discharge, LV systolic function improved to 39% and there were no findings concerning for coronary artery thrombosis or fistula repair failure. However some patients can develop heart failure, angina, and arrhythmia due to significant intracardiac shunt or coronary steal phenomenon. It is often clinically silent.
The primary endpoint consisted of a composite of all-cause mortality, MI, stroke, coronary revascularization, or hospitalization for unstable angina. The primary non-inferiority endpoint was MACCE (a composite of cardiac death, MI, ischaemic stroke, stent thrombosis, or target vessel revascularisation). in the medical therapy group.
Takotsubo is a sudden event, not one with crescendo angina. 9 This dissociation between the degree of stenosis and the propensity to provoke an acute coronary syndrome helps to explain why myocardial infarction often occurs without being heralded by the demand-induced symptoms of angina that would result from a high-grade stenosis.
12,16 In 2017, CANTOS (Canakinumab Anti-inflammatory Thrombosis Outcomes Study) provided proof-of-principle that inflammation inhibition in the absence of lipid lowering can significantly reduce cardiovascular event rates and helped to define the interleukin-1 (IL-1) to IL-6 to CRP pathway as a central target in CV disease.16
The reappearance of de Winter's pattern caused by acute stent thrombosis: A case report. He presented with recent angina that evolved into a 3-hour episode of persistent CP unrelieved by rest. Prominent T wave and J-point depression in the precordial leads associated with ST-segment elevation in lead aVR. Am J Emerg Med. 2022.01.006 6.
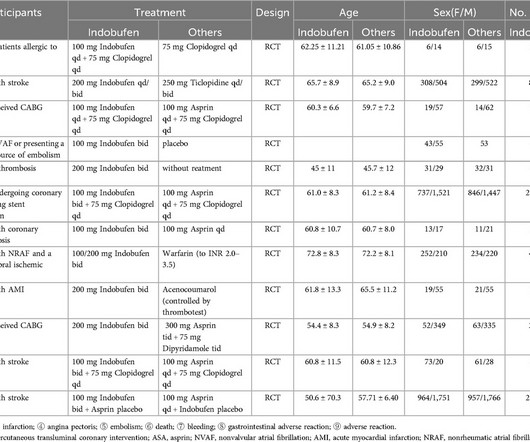
The primary focus is on the incidence of major adverse cardiovascular events (MACE), thrombosis, bleeding events, and adverse reactions. However, the effects of both treatments on efficacy outcomes, including MACE, myocardial infarction, angina, mortality, and thrombotic events, were similar.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content