This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
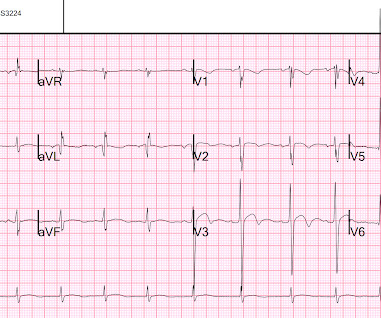
Patient still not having chest pain however this is more concerning for OMI/STEMI. Patient is pain free and clearly has Wellens' syndrome: 1) pain free episode following an episode of angina, typical Pattern A (biphasic, terminal T-wave inversion with an initial upsloping ST Segment) findings, preserved R-waves. Aspirin given.
Will evolve into STEMI by prothrombotic trigger of lytic agent ECG will get normalised with clinical stability in some Nothing happens. In addition, the criteria require the absence of precordial Q waves, the presence of history of angina, and normal or slightly elevated cardiac serum markers. ECG will remain same.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction.
Here is the prehospital ECG, with pain: Hyperacute anterolateral STEMI The medics had activated the cath lab and the patient went for angiogram and had a 95% stenotic LAD with TIMI-3 flow. When there is extremely brief ischemia, as in this case , or this case , it may entirely reverse, especially in unstable angina (negative troponins).
A middle-aged woman had intermittent angina for 48 hours, then onset of constant, crushing chest pain for 1.5 cm diameter in the apex The presence of thrombus led the clinicians to state that this was a "late presentation STEMI." hours when she called 911. LV Thrombus , 1.5 0 0 1 95 544 MMRF 4 1 638 14.0 Methods: Vermeer et al.
Angiographic and clinical characteristics of patients with unstable angina showing and ECG pattern indicating critical narrowing of the proximal LAD coronary artery. See these posts for Wellens' mimics: Pseudo-Wellens' Syndrome due to Left Ventricular Hypertrophy (LVH) Anterior STEMI? It even meets STEMI criteria: 2.5
A comparison of electrocardiographic changes during reperfusion of acute myocardial infarction by thrombolysis or percutaneous transluminal coronary angioplasty. So even a massive STEMI, if it reperfused quickly, can result in a relatvely low troponin (in contrast to the next case!) Wehrens XH, Doevendans PA, Ophuis TJ, Wellens HJ.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.













Let's personalize your content