This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Does heparin - LMWH or unfractionated heparin - benefit the patient with a pretty good story for angina with a bump in their troponin and some ST depression in the lateral leads? We’re expected to routinely give heparin for all these NSTEMI and unstable angina patients with any ischemic changes seen on the ECG, right? But should we?
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
See my formula for differentiating anterior LV aneurysm (that is to say, persistent ST elevation after old MI) from acute anterior STEMI. Both support acute anterior STEMI. This is clearly an oversimplification, as many patients have pain for very long periods that is not irreversible infarction but rather ongoing angina.
The post EM Quick Hits 4 Acetaminophen Overdose & Warfarin Interaction, Dental Infections, MTP RABT Score, Statins for STEMI, Cricothyrotomy Tips appeared first on Emergency Medicine Cases.
This is a 45 yo male who had an inferior STEMI 6 months prior, was found to have severe LAD and left main disease, and was supposed to be set up for CABG a few weeks later, but did not follow up. But it could be anterior STEMI. 40% of anterior STEMI has upward concavity in all of leads V2-V6. is likely anterior STEMI).
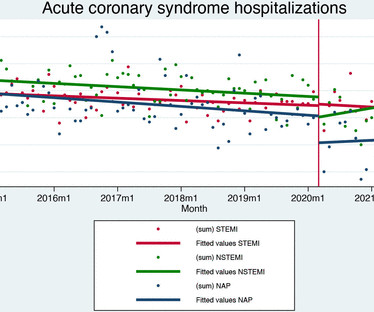
Data on 21 001 patients were included (7057 ST-elevation myocardial infarction (STEMI), 7649 non-ST elevation myocardial infarction (NSTEMI) and 6295 unstable angina). In patients with STEMI, the pandemic did not affect reperfusion rates (0.29%, (95% CI) –1.5%
This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. Therefore this is " Transient ST Elevation Unstable Angina." As there was ruptured plaque, this is NOT Prinzmetal's angina. Here are many other cases of Unstable Angina , in spite of Eugene Braunwald's Requiem for Unstable Angina.
Patient still not having chest pain however this is more concerning for OMI/STEMI. Patient is pain free and clearly has Wellens' syndrome: 1) pain free episode following an episode of angina, typical Pattern A (biphasic, terminal T-wave inversion with an initial upsloping ST Segment) findings, preserved R-waves. Aspirin given.
with ST elevated myocardial infarction (STEMI), 3.41% with unstable angina, 0.56% with stable angina, and 0.11% were diagnosed with various types of arrhythmias. Approximately 48.5% of the patients were diagnosed with non-ST elevated myocardial infarction (NSTEMI), 36.8%
If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia. The cardiologist recognized that there were EKG changes, but did not take the patient for emergent catheterization because the EKG was “not meeting criteria for STEMI”.
Inferior STEMI without inferior ST elevation. The development of an inferior-posterior STEMI, from prehospital to hospital Case 6. A Case of Clinical Unstable Angina in the ED This case shows how hyperacute is only relative to the baseline T-waves. Is this STEMI? Subtle Inferoposterolateral STEMI
Thus, the patient does not (yet) get a formal diagnosis of MI and must be called unstable angina unless further troponins return above the 99th percentile. On the basis of unresolved angina, cardiology decided to perform rescue PCI. Medically refractory angina should have immediate angiography, but this only happens 6.4%
Will evolve into STEMI by prothrombotic trigger of lytic agent ECG will get normalised with clinical stability in some Nothing happens. In addition, the criteria require the absence of precordial Q waves, the presence of history of angina, and normal or slightly elevated cardiac serum markers. ECG will remain same.
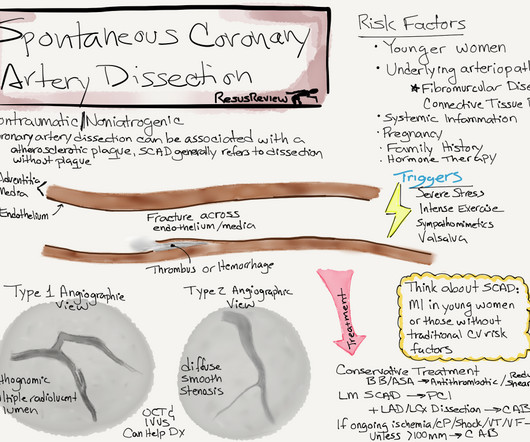
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction.
The patient was given aspirin, heparin, morphine, and ondansetron and and transferred to a PCI-capable facility for a diagnosis of "unstable angina" with dynamic ECG changes. The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Is there STEMI? What is the rhythm? Moffat, M.
This has important clinical significance , as many successfully lysed STEMI patient might have minimal segments of dissection/deep plaque fissures. , may be misdiagnosed as post infarct angina. Mind you, even if it occurs, it is atypical, continuous, non-anginal if flow is unaffected, and not relieved by nitro-glycerine.
It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI. A mong patients with STEMI, ventricular septal rupture is the most common and free wall rupture is the least common.
We present the cumulative percutaneous coronary intervention (PCI) data of all comers (stable angina and acute coronary syndromes [ACS]) who presented to Hadi Clinic between January 2018 and December 2020. The radial approach was used in 544/567 (95.94%), the average SYNTAX score was 34.8 ± 9.6, and the average number of stents 2.6.
This study investigates the relationship between baseline 5-HTP levels and the incidence of major adverse cardiovascular events (MACE) in patients who have experienced ST-elevation myocardial infarction (STEMI).Objective:Our Conclusion:Higher 5-HTP levels are independently associated with a reduced risk of MACE in patients after STEMI.
DECISION-CTO,EURO-CTO,EXPLORE,IMPACTOR) Opening a CTO, for reasons other than angina (i.e. One more remote risk in CTO is, acute collateral shutdown causing STEMI/NSTEMI. for relief of dyspnea or improving functional capacity) is largely conjectural and based on randomly accrued data backed by poor interpretation.
You've read in my previous posts that I have a lot of evidence that Wellens' represents spontaneously reperfused STEMI in which the STEMI went unrecorded. New ST elevation diagnostic of STEMI [equation value = 25.3 Silent ischemia as a marker for early unfavorable outcomes in patients with unstable angina.
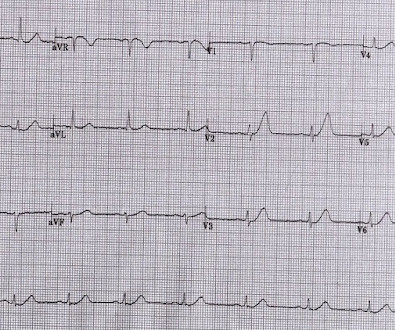
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
This appears to be a classic Wellens' ECG, Pattern A, with terminal T-wave inversion in V2-V4, preserved R-waves, and it appears to be Wellens' syndrome, as it occurred after resolution of typical angina pain. Wellens' syndrome represents the aftermath of an unrecorded occlusion (STEMI) with spontaneous reperfusion.
But beware the few false negatives, especially when there are hyperacute T-waves but no ST elevation (see Case 2 below): Formula to differentiate Normal Variant ST Elevation (Early Repolarization) from Anterior STEMI. 2 or 3 do not rule out unstable angina, even in the era of high sensitivity troponin: this study by Thelin et al.
Types of ACS include stable angina 5.3% (n=8), unstable angina 24% (n=36), NSTEMI 28.7% (n=43), and STEMI 24% (n=36). The MACE was assessed 30-days after PPCI through phone calls with patients and confirmed from medical records.Results:The study included 150 patients with ACS, 82.7% (n= 124) of them were males.
Here is the prehospital ECG, with pain: Hyperacute anterolateral STEMI The medics had activated the cath lab and the patient went for angiogram and had a 95% stenotic LAD with TIMI-3 flow. When there is extremely brief ischemia, as in this case , or this case , it may entirely reverse, especially in unstable angina (negative troponins).
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
While this ECG is negative for “posterior STEMI”, the resolution of anterior ST depression (accompanied by the troponin elevation) confirms posterior OMI with spontaneous reperfusion. The second opportunity to make the diagnosis and expedite angiography was missed because the ECG never met STEMI criteria and continued to be labeled ‘normal.’
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. He does have a recently diagnosed PE, and has not been taking his anticoagulation due to cost. He had a previous ECG on file: Proving the findings are new The cath lab was activated. He was given aspirin and sublingual nitro and the pain resolved.
A middle-aged woman had intermittent angina for 48 hours, then onset of constant, crushing chest pain for 1.5 cm diameter in the apex The presence of thrombus led the clinicians to state that this was a "late presentation STEMI." hours when she called 911. LV Thrombus , 1.5 0 0 1 95 544 MMRF 4 1 638 14.0
The HEART and EDACS scores are helpful to risk stratify patients with chest pain, but they hinge on accurate ECG interpretation: a low score doesn’t apply if the ECG shows STEMI(+)OMI, and shouldn’t be used for STEMI(-)OMI or OMI reperfusion either 2. Specifying the level is more accurate, evidence-based and safe 3.
Takotsubo is a sudden event, not one with crescendo angina. 9 This dissociation between the degree of stenosis and the propensity to provoke an acute coronary syndrome helps to explain why myocardial infarction often occurs without being heralded by the demand-induced symptoms of angina that would result from a high-grade stenosis.
Angiographic and clinical characteristics of patients with unstable angina showing and ECG pattern indicating critical narrowing of the proximal LAD coronary artery. See these posts for Wellens' mimics: Pseudo-Wellens' Syndrome due to Left Ventricular Hypertrophy (LVH) Anterior STEMI? It even meets STEMI criteria: 2.5
Later, she developed chest pain again, and had this ECG recorded: Obvious Anterior OMI that is also a STEMI Coronary angiogram- --Right dominant coronary artery system --The left main artery was normal in appearance and free of obstructive disease. --The Thus, Wellens' syndrome should be thought of as a transient OMI or transient STEMI.
Despite ongoing chest discomfort and an uptrending troponin, he never meets STEMI criteria. As has been mentioned numerous times on this site and is redemonstrated here: expert, subjective ECG interpretation is superior to STEMI criteria. Despite having acute coronary occlusion by cath, his ECGs never met STEMI criteria.
ECG Blog #337 — The importance of the new OMI ( vs the old STEMI ) Paradigm ( and My Comment in the July 31, 2020 post in Dr. Smith's ECG Blog ). == A DDENDUM ( 7/15/2023 ) : The original 3 ECGs in today's case were recorded using the Cabrera lead format.
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). He presented with recent angina that evolved into a 3-hour episode of persistent CP unrelieved by rest. As per Drs.
It is equivalent to a transient STEMI. Not much, but studies of STEMI and NonSTEMI show that about 70% of those diagnosed with STEMI have a peak troponin I above 10 ng/mL and that about 70% of those diagnosed with NonSTEMI have a peak troponin I below 10 ng/mL. Again, cath lab was not activated. Int J Cardiol. 2016;207:341–348.
They recorded a prehospital ECG and diagnosed STEMI and activated the cath lab prehospital. The patient did not report angina with stress. male with a history of HTN and ETOH developed squeezing epigastric abdominal pain with associated vomiting and diaphoresis, followed by a syncopal episode which lasted about 10 seconds.
A middle aged patient who was 3 weeks s/p STEMI came from cardiac rehab where he developed some chest pain, dyspnea and weakness on the treadmill. There is no acute STEMI. This is diagnostic of recent, reperfused STEMI. This is diagnostic of recent, reperfused STEMI. Acute STEMI would have upright T-waves.
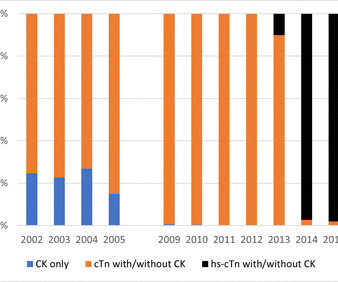
Using person-linked hospitalisation data, we compared International Classification of Diseases (ICD)-coded data with biomarker-classified admission rates for ST-segment elevation MI (STEMI), non-STEMI (NSTEMI) and unstable angina (UA) in Western Australia (WA). Results There were 37 272 ACS admissions in 30 683 patients (64.2%
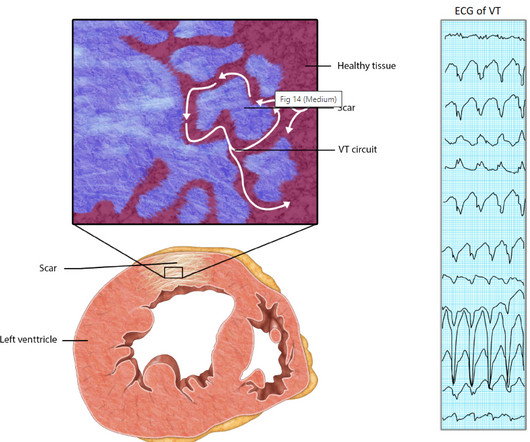
There is a problem here too ,even critical Ischemia with high grade unstable angina rarely trigger a VT but STEMI seems to have the exclusive rights to trigger it , by its ability to produce acute transmural ischemia.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.












































Let's personalize your content