This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Thus, the patient does not (yet) get a formal diagnosis of MI and must be called unstable angina unless further troponins return above the 99th percentile. On the basis of unresolved angina, cardiology decided to perform rescue PCI. Although it is statistically unlikely, multiple plaque ruptures are possible. Heitner et al.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction.
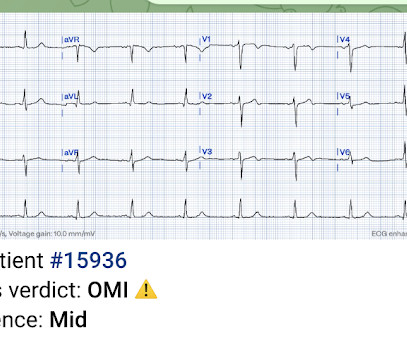
Patient is pain free and clearly has Wellens' syndrome: 1) pain free episode following an episode of angina, typical Pattern A (biphasic, terminal T-wave inversion with an initial upsloping ST Segment) findings, preserved R-waves. Angiography : --Culprit for the patient's unstable angina/Wellen syndrome is a ruptured plaque in the mid LAD. --As
The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. Therefore it means acute type 1 ACS plaque rupture with impeded flow and impending full occlusion until proven otherwise.
LAD plaque with 0-25 percent stenosis. INTERVENTION * Successful angioplasty and stenting (drug eluting) of the mid LAD * Successful angioplasty of the ostial 1st diagonal Learning points: 1. Now, with elevated troponins, Wellens' syndrome is likely. A CT Coronary angiogram was ordered. CAD-RADS category 1. --No
The lesion was stented. Prog- nostic impact of spontaneous coronary artery dissection in young female patients with acute myocardial infarction: a report from the Angina Pecto- ris-Myocardial Infarction Multicenter Investigators in Japan. It seems that there was some uncertainly about this. Int J Cardiol. 2016;207:341–348.
The logic of stenting obstructed coronary arteries is simple. A stent unblocks the artery. Subscribe now Stenting stable coronary artery disease has not been convincingly proven to reduce the risk of future heart attacks or death 1. But coronary stenting is not the only way to reduce symptoms of angina.
This was diagnosed by IVUS (intravascular ultrasound) as a ruptured plaque. It was stented. Therefore this is " Transient ST Elevation Unstable Angina." As there was ruptured plaque, this is NOT Prinzmetal's angina. So Unstable Angina still exists [even with high sensitivity (hs) troponins]. Mokhtari et al.
She was found to have a 100% occlusion of her Mid LAD just after the takeoff of D1 - which was reperfused and stented. Here is another similar case: Dynamic T-wave inversion (apparent Wellens' waves), all troponins negative: Unstable Angina Sam's Learning Points : 1. Unstable Angina still exists. This is very dangerous thinking.
The primary endpoint consisted of a composite of all-cause mortality, MI, stroke, coronary revascularization, or hospitalization for unstable angina. The primary non-inferiority endpoint was MACCE (a composite of cardiac death, MI, ischaemic stroke, stent thrombosis, or target vessel revascularisation). in the medical therapy group.
I have said before, treating angina with morphine and continuing non-emergent management is like taking the batteries out of an actively alarming smoke detector during a house fire and going back to sleep. As per Dr. Frick use of intravascular imaging ( IVUS or OCT ) could have helped to find plaque rupture and identify the "true" culprit.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


















Let's personalize your content