This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Coronary artery spasm (CAS), or Prinzmetal angina, is a recognised cause of myocardial ischaemia in non-obstructed coronary arteries which typically presents with anginal chest pain. This case report describes an atypical presentation of CAS in a 68-year-old white British male with cardiovascular riskfactors.
Artery Damage : Hypertension damages the inner lining of your arteries, making them less elastic and more prone to plaque buildup. This condition, called atherosclerosis, narrows the arteries, restricting blood flow and increasing the risk of heart attacks and strokes.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction.
The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia.
Immune-mediated inflammatory diseases (IMIDs) are recognised riskfactors for accelerated atherosclerotic cardiovascular disease (CVD), particularly in younger individuals and women who lack traditional CVD riskfactors.
Given the consistency of the clinical profile with typical angina, associated riskfactors, and abnormal ECG findings, a cardiology consult was promptly requested. Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates.
I quickly reviewed the patient’s records and saw that she was a 53 year old woman with a history of BMI 40, but no other identifiable riskfactors for coronary artery disease. Learning Points: Type 1 MI is the type we are most familiar with: rupture of atherosclerotic plaque with production thrombus or platelet fibrin aggregates.
Sustained inflammation can damage your blood vessels, leading to atherosclerosis (plaque buildup) and increasing your risk of heart attack and stroke. This can lead to chest pain (angina) and increase your risk of heart attack or stroke, especially if you already have underlying heart disease.
ET Murphy Ballroom 4 Health 360x Registry: Scalable Workforce for Equitable Access to Point of Care Decentralized Clinical Trials Prevalence of Cardiovascular Disease and RiskFactors Among National Football League Alumni and Their Family Members: Results from the Huddle Study Hózhó (Heart Failure Optimization at Home to Improve Outcomes): A Pragmatic (..)
She had some very minor plaque but certainly nothing that could explain the heart attack and therefore she was discharged with a diagnosis of MINOCA i.e Genetics and physiological stress are also riskfactors. She agreed and we performed an angiogram and we were fully expecting a blockage but interestingly there weren’t any.
She had zero CAD riskfactors. SCAD occurs in patients with few or non-traditional cardiovascular riskfactors. There has been multiple factors associated with SCAD that may predispose to a weaken arterial wall, fibromuscular dysplasia (FMD) and pregnancy being the most common 2,5. Int J Cardiol. 2016;207:341–348.
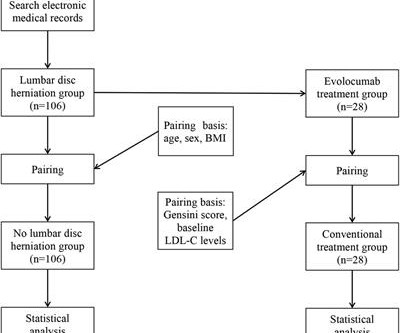
Objective Assessing the impact of lumbar disc herniation (LDH) on the plaque burden of coronary atherosclerosis is our objective. Methods In this study, a total of 212 patients (age 46–80 years) with unstable angina (UA) who underwent coronary angiography (CAG) in our hospital from January 2018 to July 2022 due to UA were included.
Atherosclerotic cardiovascular disease (ASCVD), caused by plaque buildup in arterial walls, is one of the leading causes of disability and death worldwide.1,2 3 Patients with ASCVD are at a higher risk for major adverse cardiovascular events (MACE) including heart attack or myocardial infarction (MI), stroke, and cardiovascular (CV) death.4
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



















Let's personalize your content