This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Coronary artery spasm (CAS), or Prinzmetal angina, is a recognised cause of myocardial ischaemia in non-obstructed coronary arteries which typically presents with anginal chest pain. This case report describes an atypical presentation of CAS in a 68-year-old white British male with cardiovascular risk factors.
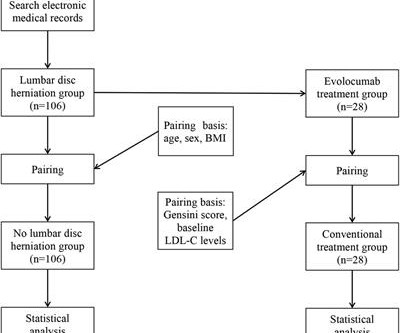
Objective Assessing the impact of lumbar disc herniation (LDH) on the plaque burden of coronary atherosclerosis is our objective. Methods In this study, a total of 212 patients (age 46–80 years) with unstable angina (UA) who underwent coronary angiography (CAG) in our hospital from January 2018 to July 2022 due to UA were included.
Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardial infarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque. The pathologist may see a plaque that constitutes, for example, 50% of the cross-sectional area.
Artery Damage : Hypertension damages the inner lining of your arteries, making them less elastic and more prone to plaque buildup. Coronary Artery Disease (CAD) : High blood pressure accelerates the development of CAD by promoting the buildup of plaques in the coronary arteries.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction.
Thus, the patient does not (yet) get a formal diagnosis of MI and must be called unstable angina unless further troponins return above the 99th percentile. On the basis of unresolved angina, cardiology decided to perform rescue PCI. Although it is statistically unlikely, multiple plaque ruptures are possible. Heitner et al.
In a patient with CAD, atheromatous plaques build inside the coronary arteries, reducing the flow of oxygen-rich blood to the heart muscle by narrowing or blocking the arteries. The patient may then experience deadly angina, myocardial fraction, or heart attack.
This has important clinical significance , as many successfully lysed STEMI patient might have minimal segments of dissection/deep plaque fissures. , may be misdiagnosed as post infarct angina. Kim N Engl J Med 2020; 383:2358-2370 Next query What is the difference between plaque fissure and coronary arterial dissection?
Possible etiologies (depending on your definition) include: plaque rupture with spontaneous recanalization, coronary artery vasospasm, spontaneous coronary artery dissection, or other rarer causes. In addition, his cardiologist suspected vasospastic angina and therefore started amlodipine. The name is self-explanatory.
Patient is pain free and clearly has Wellens' syndrome: 1) pain free episode following an episode of angina, typical Pattern A (biphasic, terminal T-wave inversion with an initial upsloping ST Segment) findings, preserved R-waves. Angiography : --Culprit for the patient's unstable angina/Wellen syndrome is a ruptured plaque in the mid LAD. --As
Whether stenting a narrowed coronary artery improves symptoms such as chest pain (angina) or shortness of breath is a very different question. Share Angina The classic definition of angina involves the sensation of tightness in the centre of the chest that is brought on with exertion and is relieved with rest. The result?
Given the consistency of the clinical profile with typical angina, associated risk factors, and abnormal ECG findings, a cardiology consult was promptly requested. Category 1 : Sudden narrowing of a coronary artery due to ACS (plaque rupture with thrombosis and/or downstream showering of platelet-fibrin aggregates. Severe Hypoxia b.
The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia.
There was no antecedent angina. The left system showed no disease in the left main stem, but mild plaque disease in the dominant left circumflex artery. Clinical introduction Vignette A man in his 40s presented to our emergency department with sudden onset of severe central chest pain radiating to his left arm.
Here is another similar case: Dynamic T-wave inversion (apparent Wellens' waves), all troponins negative: Unstable Angina Sam's Learning Points : 1. For example, a coronary plaque ruptures: the vessel can undergo occlusion, spontaneous reperfusion, maybe reocclusion, again reperfusion, etc. Unstable Angina still exists.
Reflective of the critical role that inflammation plays in the formation, progression and rupture of atherosclerotic plaques, research into immune mechanisms of CVD has led to the identification of a range of therapeutic targets that are the subject of ongoing clinical trials.
In addition, the criteria require the absence of precordial Q waves, the presence of history of angina, and normal or slightly elevated cardiac serum markers. It is generally believed it is more of a mechanical plaque lesion. Wellens is a glorified subset of ACS. It can be referred to as an ACS in a confused state of evolution.
Sustained inflammation can damage your blood vessels, leading to atherosclerosis (plaque buildup) and increasing your risk of heart attack and stroke. This can lead to chest pain (angina) and increase your risk of heart attack or stroke, especially if you already have underlying heart disease.
This was diagnosed by IVUS (intravascular ultrasound) as a ruptured plaque. Therefore this is " Transient ST Elevation Unstable Angina." As there was ruptured plaque, this is NOT Prinzmetal's angina. It is just as dangerous, as there is a ruptured plaque with thrombus (which lysed) in the proximal LAD.
The primary endpoint consisted of a composite of all-cause mortality, MI, stroke, coronary revascularization, or hospitalization for unstable angina. These patients were identified to have non-flow-limiting vulnerable coronary plaques through intracoronary imaging. of patients in the PCI group compared to 3.4%
Atherosclerotic cardiovascular disease (ASCVD), caused by plaque buildup in arterial walls, is one of the leading causes of disability and death worldwide.1,2 7 Research has shown inflammation plays a significant role in the development of atherosclerosis and ASCVD,8-10 and even the formation of plaque.11 4 In the U.S.
For example, if a coronary artery becomes blocked due to plaque buildup (a condition known as coronary artery disease), the heart muscle may not receive enough oxygen, leading to chest pain (angina) or, in more severe cases, a heart attack. Any interruption in this process can result in serious consequences.
Learning Points: Type 1 MI is the type we are most familiar with: rupture of atherosclerotic plaque with production thrombus or platelet fibrin aggregates. Serial EKG is very high yield diagnostic test in patients with stuttering angina. But not all OMI is atherosclerotic in nature.
Takotsubo is a sudden event, not one with crescendo angina. To prove there is no plaque rupture, you need to do intravascular ultrasound (IVUS). An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!! I need to innoculate you against the subsequent opinions below. It can only be seen by IVUS. MINOCA has many etiologies.
With time, fat and cholesterol can get trapped in the areas of wear and tear and cause plaque formation. The plaques can damage us in 2 ways. Firstly the plaque may continue to build up and cause actually restrict blood from getting to the heart muscle and this often presents with symptoms of chest tightness on exertion or angina.
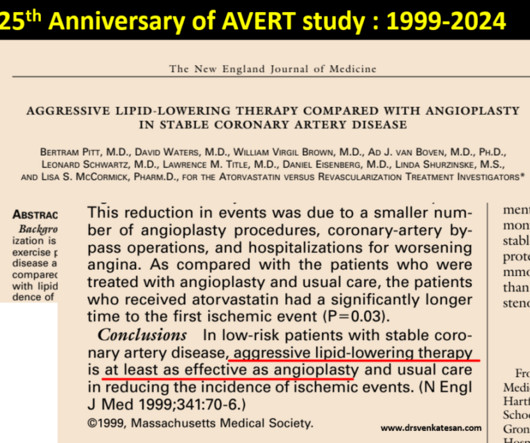
This study tested PTCA vs with a single lipid lowering drug in terms of plaque regression. Bertram Pitt and his team scripted this from the Department of Medicine, University of Michigan School of Medicine, Ann Arbor, USA. One can’t expect even in your dreams a study like this would be be done in the future.
ET Main Tent (Hall B1) A Selective Aldose Reductase Inhibitor (at-001) For the Treatment of Diabetic Cardiomyopathy: Primary Results of the Phase 3 Randomized Controlled ARISE-HF Study Efficacy and Safety of Ninerafaxstat, a Novel Cardiac Mitotrope, in Patients with Symptomatic Nonobstructive Hypertrophic Cardiomyopathy: Results of IMPROVE-HCM Topical (..)
She had some very minor plaque but certainly nothing that could explain the heart attack and therefore she was discharged with a diagnosis of MINOCA i.e MINOCA – When a heart attack is not a heart attack Keywords: MINOCA; MI with normal coronary arteries; Coronary vasospasm; Microvascular angina; Syndrome X; Prinzmetal angina.
SHASTA-2—looks at a new medicine plozasiran on the treatment of hypertriglyceridemia SMART Trial—a head-to-head trial of the self-expanding vs. a balloon-expanding TAVR DanGer Shock—brings equipoise to how cardiogenic shock is treated in general, looking at the use of a transvalvular mico-axial flow pump in patients who have infarct or heart attack (..)
Therefore it means acute type 1 ACS plaque rupture with impeded flow and impending full occlusion until proven otherwise. He presented with recent angina that evolved into a 3-hour episode of persistent CP unrelieved by rest. Then, the patients third ECG showed a very rare combination of de Winter T waves happening during LBBB.
LAD plaque with 0-25 percent stenosis. Now, with elevated troponins, Wellens' syndrome is likely. A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD CAD-RADS category 1. --No Given that the patient has had an abnormal elevated troponin, would suggest a Cardiology evaluation.
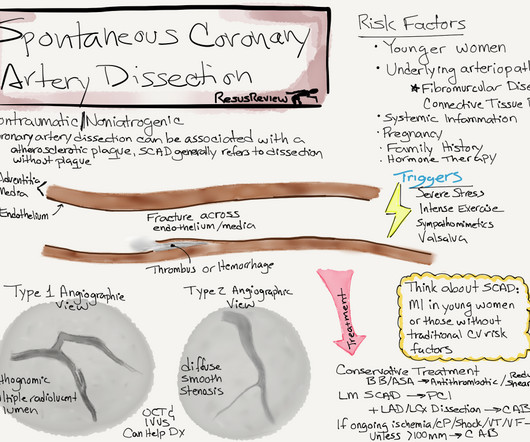
Prog- nostic impact of spontaneous coronary artery dissection in young female patients with acute myocardial infarction: a report from the Angina Pecto- ris-Myocardial Infarction Multicenter Investigators in Japan. SCAD occurs in patients with few or non-traditional cardiovascular risk factors. Int J Cardiol. 2016;207:341–348. 2016.01.188.
BACKGROUND:Recent studies have shown that vasospastic angina (VSA) is associated with myocardial bridge (MB) and pericoronary adipose tissue inflammation. Coronary plaques were qualitatively classified as noncalcified or calcified plaques in each vessel. Factors associated with VSA included male sex (74.5% versus 51.7%,P=0.01),
We investigated potential associations between cumulative atherosclerotic plaque burden quantified using the Gensini score, novel invasive indices of coronary microvascular function (microvascular resistance reserve (MRR); resistive reserve ratio (RRR)) and related INOCA endotypes. –11.0)), vasospastic angina (VSA) (4.5 (2.0–10.0)),
Additionally, the ongoing ORBITA-2 trial examines the use of percutaneous coronary intervention (PCI) for stable angina, offering valuable insights into procedural benefits and outcomes.
I have said before, treating angina with morphine and continuing non-emergent management is like taking the batteries out of an actively alarming smoke detector during a house fire and going back to sleep. As per Dr. Frick use of intravascular imaging ( IVUS or OCT ) could have helped to find plaque rupture and identify the "true" culprit.
One big chunk of ACS-UA is secondary UA where there is increased demand as in stable angina with tachycardia*. In these patients there is no plaque triggered ACS. For example, in a febrile patient who has associated HT, anemia, etc.,
Nevertheless, the operator performed intravascular ultrasound and saw erupted calcium nodule consistent with plaque erosion. Even though guidelines say that patients with high-risk features, refractory angina, instability, etc. As you can see, the lesion is not very angiographically impressive , more on this below.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.







































Let's personalize your content