This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
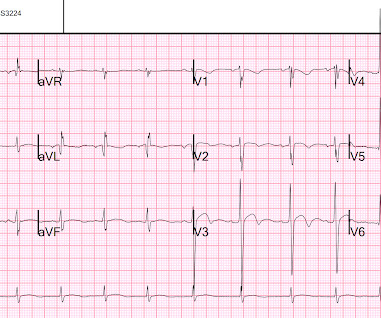
Patient is pain free and clearly has Wellens' syndrome: 1) pain free episode following an episode of angina, typical Pattern A (biphasic, terminal T-wave inversion with an initial upsloping ST Segment) findings, preserved R-waves. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction.
In my experience, all Wellens' with significant myocardialinfarction have evolution from type A waves to type B waves over 6-24 hours' time , so that the presence of type A or type B waves, I believe, are simply a matter of the timing of recording and the rapidity of evolution. Lessons: 1. de Zwaan C., Janssen J.H.A., de Zwaan C.,
Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardialinfarction. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. Am Heart J. Am Heart J.
A middle-aged woman had intermittent angina for 48 hours, then onset of constant, crushing chest pain for 1.5 Appearance of abnormal Q waves early in the course of acute myocardialinfarction: implications for efficacy of thrombolytic therapy. hours when she called 911. These do NOT indicate late, subacute MI. Raitt MH, et al.
The TIMI (Thrombolysis in MyocardialInfarction) Study Group is a Division of Cardiovascular Medicine at the esteemed Brigham and Women’s Hospital and Harvard Medical School. Anish Koka, MD @anish_koka This was driven almost entirely by myocardialinfarction / need for revascularization.
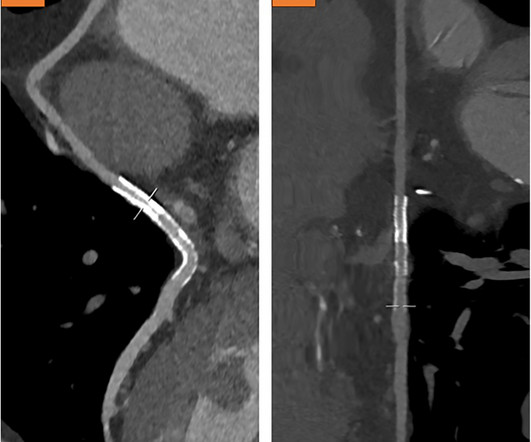
This case report discusses a 75-year-old male patient who presented with angina and shortness of breath due to thrombus formation in a venous graft 20 years after CABG. Initial diagnostics indicated non-ST-elevation myocardialinfarction, leading to immediate intervention.
A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. Am Heart J 2000;139(3):4306. Br, Johan H.A.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











Let's personalize your content