This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A middle-aged man complained of 15 minutes of classic angina that resolved upon arrival to the ED. So this is indeed diagnostic of myocardialinfarction. Not immediately, at least, because this is NOT diagnostic of ACUTE (occlusion) myocardialinfarction (Acute OMI). Angiogram: Widely patent RCA and LAD stents.
of the patients were diagnosed with non-ST elevated myocardialinfarction (NSTEMI), 36.8% with ST elevated myocardialinfarction (STEMI), 3.41% with unstable angina, 0.56% with stable angina, and 0.11% were diagnosed with various types of arrhythmias. Approximately 48.5% and 1.3%, respectively.
Patient is pain free and clearly has Wellens' syndrome: 1) pain free episode following an episode of angina, typical Pattern A (biphasic, terminal T-wave inversion with an initial upsloping ST Segment) findings, preserved R-waves. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction.
Drug‐eluting stents have been shown to be superior to bare‐metal stents in patients with HBR, even when patients were given abbreviated periods of dual antiplatelet therapy (DAPT). Short DAPT has not been evaluated with the EluNIR ridaforolimus‐eluting stent.
The impact of this narrowing can ultimately result in angina (chest pain), which has been shown to double the risk of major cardiovascular events,1 as well as myocardialinfarction ( heart attack ) or even death. Use Heart to Act on Angina. Available at: [link]. Accessed May 2024.
So there is probability of myocardial injury here (and because it is in the correct clinical setting, then myocardialinfarction.) Thus, the patient does not (yet) get a formal diagnosis of MI and must be called unstable angina unless further troponins return above the 99th percentile. Repeat ECG is shown below.
A stent was placed. In my experience, all Wellens' with significant myocardialinfarction have evolution from type A waves to type B waves over 6-24 hours' time , so that the presence of type A or type B waves, I believe, are simply a matter of the timing of recording and the rapidity of evolution. Lessons: 1. de Zwaan C.,
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. 1] European guidelines add "regardless of biomarkers". But only 6.4% Clin Cardiol 2022 4. Herman, Meyers, Smith et al.
We present the cumulative percutaneous coronary intervention (PCI) data of all comers (stable angina and acute coronary syndromes [ACS]) who presented to Hadi Clinic between January 2018 and December 2020. and the average number of stents 2.6. The radial approach was used in 544/567 (95.94%), the average SYNTAX score was 34.8 ± 9.6,
The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia.
EMPACT-MI 1 ( NCT04509674 ) studied the effects of empagliflozin in patients who have experienced myocardialinfarction (MI). The primary endpoint consisted of a composite of all-cause mortality, MI, stroke, coronary revascularization, or hospitalization for unstable angina. Here is our curated list of the top sessions.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. A New ST-segment elevation myocardialinfarction equivalent pattern? An Impella was placed for cardiac output augmentation.
As hours go by, these T inversions always evolve , [unless 1) there is re-occlusion, in which case they go upright and become hyperacute, with or without additional ST elevation, ("pseudonormalize") or 2) no infarction at all (negative troponin, true unstable angina with dynamic T-waves, in which they may normalize). It was stented.
A middle-aged woman had intermittent angina for 48 hours, then onset of constant, crushing chest pain for 1.5 Appearance of abnormal Q waves early in the course of acute myocardialinfarction: implications for efficacy of thrombolytic therapy. It was treated with and dual "kissing balloons" and drug eluting stents.
It was stented. Therefore, this does not meet the definition of myocardialinfarction ( 4th Universal Definition of MI ), which requires at least one troponin above the 99% reference range. Therefore this is " Transient ST Elevation Unstable Angina." As there was ruptured plaque, this is NOT Prinzmetal's angina.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
At the bottom of the post, I have re-printed the section on aVR in my article on the ECG in ACS from the Canadian Journal of Cardiology: New Insights Into the Use of the 12-Lead Electrocardiogram for Diagnosing Acute MyocardialInfarction in the Emergency Department Case 1. Widimsky P et al. This was a 100% acute LM occlusion.
Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardialinfarction. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. Am Heart J. Am Heart J.
Typical angina was defined as a symptom complex that includes substernal chest pressure or pain that was made worse with exertion/emotional stress, and relieved by rest or nitroglycerin. Atypical angina is classified as having any two of the three symptoms, and non-anginal pain any one of the three symptoms.
In the STEMI/NSTEMI dichotomy, NSTEMI is supposed to mean non-occlusive myocardialinfarction, but this patient had transient Occlusion MI that was at risk for re-occlusion (like ‘transient STEMI’). Notice also that there is new T-wave inversion in III with upright T-wave in aVL, confirming inferior infarction.
This is diagnostic of myocardialinfarction. The lesion was stented. In middle age women, it accounts for 22-35% of all ACS presentations 1,3 , and the reported incidence of ST-elevation myocardialinfarction in this subset of patients is variable, but estimated to be between 24-50% 4. Int J Cardiol. 2016.01.188.
ng/mL This single initial troponin at this level, in the context of chest pain, is high enough to be diagnostic of acute myocardialinfarction. INTERVENTION * Successful angioplasty and stenting (drug eluting) of the mid LAD * Successful angioplasty of the ostial 1st diagonal Learning points: 1. Young women do get acute MI 2.
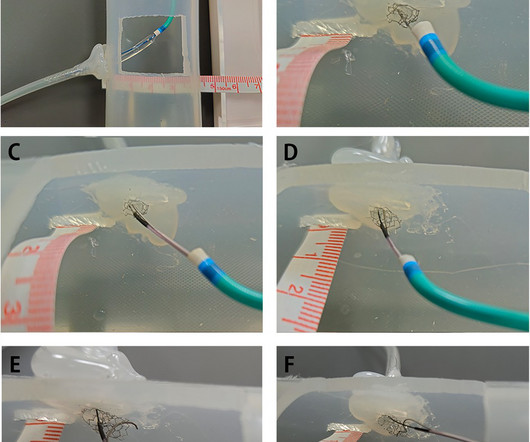
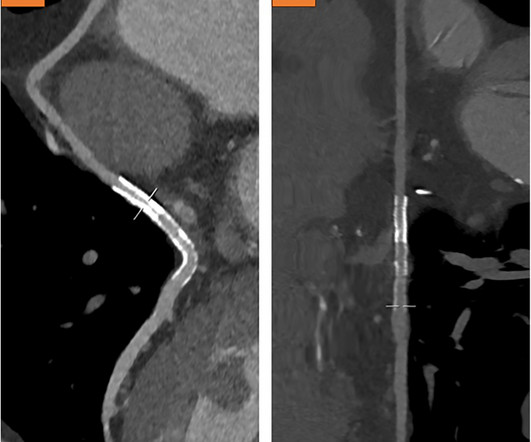
BackgroundPercutaneous coronary intervention (PCI) through the aorto-ostial coronary stent that is protruding into the aorta remains a technical challenge because of the poor coaxial alignment of the guiding catheter and the inability to advance the guidewire into the distal vessel through the stent's central lumen.
This case report discusses a 75-year-old male patient who presented with angina and shortness of breath due to thrombus formation in a venous graft 20 years after CABG. Initial diagnostics indicated non-ST-elevation myocardialinfarction, leading to immediate intervention.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content