This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
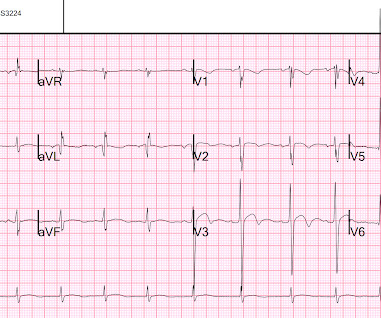
I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion. Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1]
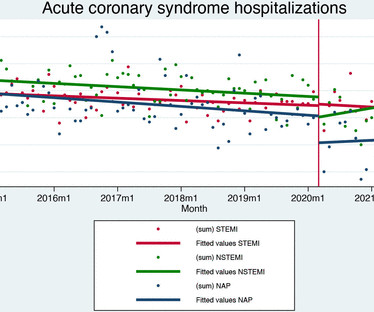
Data on 21 001 patients were included (7057 ST-elevation myocardialinfarction (STEMI), 7649 non-ST elevation myocardialinfarction (NSTEMI) and 6295 unstable angina). In patients with STEMI, the pandemic did not affect reperfusion rates (0.29%, (95% CI) –1.5%
Patient still not having chest pain however this is more concerning for OMI/STEMI. Patient is pain free and clearly has Wellens' syndrome: 1) pain free episode following an episode of angina, typical Pattern A (biphasic, terminal T-wave inversion with an initial upsloping ST Segment) findings, preserved R-waves. Aspirin given.
This is a value typical for a large subacute MI, n ormal value 48 hours after myocardialinfarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). Mechanical complications secondary to myocardialinfarction are infrequent due to most patients receiving revascularization quite rapidly.
The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia.
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardialinfarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque.
Here is the prehospital ECG, with pain: Hyperacute anterolateral STEMI The medics had activated the cath lab and the patient went for angiogram and had a 95% stenotic LAD with TIMI-3 flow. When there is extremely brief ischemia, as in this case , or this case , it may entirely reverse, especially in unstable angina (negative troponins).
So there is probability of myocardial injury here (and because it is in the correct clinical setting, then myocardialinfarction.) Thus, the patient does not (yet) get a formal diagnosis of MI and must be called unstable angina unless further troponins return above the 99th percentile. Repeat ECG is shown below.
You've read in my previous posts that I have a lot of evidence that Wellens' represents spontaneously reperfused STEMI in which the STEMI went unrecorded. New ST elevation diagnostic of STEMI [equation value = 25.3 Consequences of reocclusion after successful reperfusion therapy in acute myocardialinfarction.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
We present the cumulative percutaneous coronary intervention (PCI) data of all comers (stable angina and acute coronary syndromes [ACS]) who presented to Hadi Clinic between January 2018 and December 2020. The radial approach was used in 544/567 (95.94%), the average SYNTAX score was 34.8 ± 9.6, and the average number of stents 2.6.
While this ECG is negative for “posterior STEMI”, the resolution of anterior ST depression (accompanied by the troponin elevation) confirms posterior OMI with spontaneous reperfusion. The second opportunity to make the diagnosis and expedite angiography was missed because the ECG never met STEMI criteria and continued to be labeled ‘normal.’
Takotsubo is a sudden event, not one with crescendo angina. Such cases are classified as MINOCA (MyocardialInfarction with Non-Obstructed Coronary Arteries). I need to innoculate you against the subsequent opinions below. by making it clear to everyone that this is NOT an EKG that one sees with takotsubo cardiomyopathy.
The HEART and EDACS scores are helpful to risk stratify patients with chest pain, but they hinge on accurate ECG interpretation: a low score doesn’t apply if the ECG shows STEMI(+)OMI, and shouldn’t be used for STEMI(-)OMI or OMI reperfusion either 2. Single High-Sensitivity Cardiac Troponin I to Rule Out Acute MyocardialInfarction.
Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardialinfarction. See these posts for Wellens' mimics: Pseudo-Wellens' Syndrome due to Left Ventricular Hypertrophy (LVH) Anterior STEMI? Am Heart J.
The ECG was read as "No STEMI" and the patient was treated like an average chest pain patient (despite the fact that a chest pain patient with active pain and active subendocardial ischemia is very high risk). A New ST-segment elevation myocardialinfarction equivalent pattern? Eur J Emerg Med. 2017;24:236–242. Am J Emerg Med.
It is equivalent to a transient STEMI. This is diagnostic of myocardialinfarction. Not much, but studies of STEMI and NonSTEMI show that about 70% of those diagnosed with STEMI have a peak troponin I above 10 ng/mL and that about 70% of those diagnosed with NonSTEMI have a peak troponin I below 10 ng/mL.
ng/mL This single initial troponin at this level, in the context of chest pain, is high enough to be diagnostic of acute myocardialinfarction. Thus, Wellens' syndrome should be thought of as a transient OMI or transient STEMI. Transient STEMI is at high risk of re-occlusion. Her initial cTnI returned at 0.25
The patient was given aspirin, heparin, morphine, and ondansetron and and transferred to a PCI-capable facility for a diagnosis of "unstable angina" with dynamic ECG changes. The receiving emergency physician consulted with interventional cardiology who stated there was no STEMI. Is there STEMI? Do not treat AIVR. Moffat, M.
This study investigates the relationship between baseline 5-HTP levels and the incidence of major adverse cardiovascular events (MACE) in patients who have experienced ST-elevation myocardialinfarction (STEMI).Objective:Our years, 53 women) followed for up to 15 years.
of the patients were diagnosed with non-ST elevated myocardialinfarction (NSTEMI), 36.8% with ST elevated myocardialinfarction (STEMI), 3.41% with unstable angina, 0.56% with stable angina, and 0.11% were diagnosed with various types of arrhythmias. Approximately 48.5%
This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. Therefore, this does not meet the definition of myocardialinfarction ( 4th Universal Definition of MI ), which requires at least one troponin above the 99% reference range. No further troponins were drawn. Why is this important?
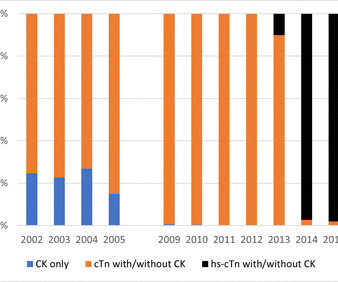
Background Since 2000, the definition of myocardialinfarction (MI) has evolved with reliance on cardiac troponin (cTn) tests. Methods We used linked hospitalisation data from all WA tertiary hospitals to identify patients with a principal diagnosis of STEMI, NSTEMI or UA between 2002 and 2016.
A middle-aged woman had intermittent angina for 48 hours, then onset of constant, crushing chest pain for 1.5 Appearance of abnormal Q waves early in the course of acute myocardialinfarction: implications for efficacy of thrombolytic therapy. hours when she called 911. These do NOT indicate late, subacute MI. Raitt MH, et al.
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline." They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
A middle aged patient who was 3 weeks s/p STEMI came from cardiac rehab where he developed some chest pain, dyspnea and weakness on the treadmill. There is no acute STEMI. This is diagnostic of recent, reperfused STEMI. This is diagnostic of recent, reperfused STEMI. Acute STEMI would have upright T-waves.
Limitations of registry data: This patient presented with STEMI (-) OMI and developed STEMI the following day. But the time that elapsed from first STEMI (+) ECG to balloon was 57 minutes, and THIS is what will be recorded for reporting to the National Cardiovascular Data Registry for purposes of quality improvement.
Smith: T waves are very hyperacute: these are a sign of ACUTE infarction, even if there are Q-waves. 50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). See Raitt et al.:
A comparison of electrocardiographic changes during reperfusion of acute myocardialinfarction by thrombolysis or percutaneous transluminal coronary angioplasty. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction. Am Heart J 2000;139(3):4306. A stent was placed.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content