This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
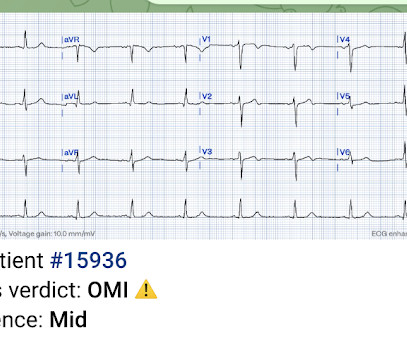
This EKG is diagnostic of transmural ischemia of the inferior wall. If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia. Transmural ischemia (as seen with the OMI findings on ECG) is not very common with demand ischemia, but is possible.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The baseline ECG is basically normal with no ischemia. In my opinion, I think it looks more like subendocardial ischemia.
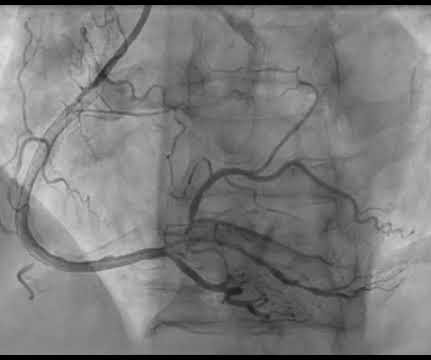
A stent was placed. For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. In this case, the duration of ischemia was so brief that there was no such evolution, and there was near-normalization. Ischemia may be so brief that Wellens' waves do not evolve 3. Lessons: 1.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chest pain radiating to the left arm, associated with nausea. 1] European guidelines add "regardless of biomarkers". But only 6.4%
The ECG in the chart was read as "no obvious ST changes," (even though no previous ECG was available) and the formal read by the emergency physicians was: "ST deviation and moderated T-wave abnormality, consider lateral ischemia." It was stented. Comment: most T-wave inversion is nonspecific, but not these ones! Gottlieb SO, et al.
Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. The lesion was stented. It they are static, then they are not due to ischemia. This is better evidence for ischemia than any other data point. Again, cath lab was not activated. Int J Cardiol.
Delayed angiogram found a 95% mid RCA occlusion that was stented. Ischemic ST-segment depression maximal in V1-V4 (versus V5-V6) of any amplitude is specific for Occlusion Myocardial Infarction (versus nonocclusive ischemia). And notice that the T-waves in V4-V6 are now back down to normal size and "bulk." JAHA 2022 Grosmaitre P et al.
The logic of stenting obstructed coronary arteries is simple. A stent unblocks the artery. Subscribe now Stenting stable coronary artery disease has not been convincingly proven to reduce the risk of future heart attacks or death 1. But coronary stenting is not the only way to reduce symptoms of angina.
The impact of this narrowing can ultimately result in angina (chest pain), which has been shown to double the risk of major cardiovascular events,1 as well as myocardial infarction ( heart attack ) or even death. Use Heart to Act on Angina. For more information: www.gehealthcare.com References: 1 World Health Federation.
It was stented. This was clearly severe subepicardial ischemia causing ST Elevation, but it was not of a long enough duration to result in measurable infarct. Therefore this is " Transient ST Elevation Unstable Angina." As there was ruptured plaque, this is NOT Prinzmetal's angina. Values: STE60V3 = 2.0, Mokhtari et al.
She was found to have a 100% occlusion of her Mid LAD just after the takeoff of D1 - which was reperfused and stented. Smith comment: T-wave inversion such as seen in the first ECG can be seen with active non-transmural ischemia. Unstable Angina still exists. Thus, unstable angina exists and can be deadly.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" That said, complete LM occlusion would be expected to have subepicardial ischemia (STE) in these myocardial territories: STE vector 1.
A middle-aged woman had intermittent angina for 48 hours, then onset of constant, crushing chest pain for 1.5 It was treated with and dual "kissing balloons" and drug eluting stents. hours when she called 911. TIMI flow is 0. Door to balloon time was 51 minutes.
Typical angina was defined as a symptom complex that includes substernal chest pressure or pain that was made worse with exertion/emotional stress, and relieved by rest or nitroglycerin. Atypical angina is classified as having any two of the three symptoms, and non-anginal pain any one of the three symptoms. This happens. But its rare!
There is low voltage in the precordium which always makes reading ischemia harder. In ACS, chest pain is the warning sign of ongoing ischemia. Smith : As Willy says, and as we've said many times before, morphine will resolve pain without resolving ischemia. ECG 1 What do you think? To me, this ECG is not diagnostic.
Unfortunately, although natively conducted beats are the best ones for evaluating ischemia, we only have a few! Moving on to ischemia , the ECG shows reperfused inferoposterolateral infarct. On Sunday, the patient complained of dyspnea and angina while ambulating. It looks like a low atrial rhythm.) Repeat ECG is shown.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content