This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
This confirms that the pain was ischemia and is now resovled. Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardial infarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque. The i nitial hs troponin I returned 75%.
This EKG is diagnostic of transmural ischemia of the inferior wall. The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). Was this resolution of demand ischemia?
Although radiation into the left arm is most classic for coronary ischemia, radiation into both arms is actually modestly more predictive ). The primary care physician's note indicates low suspicion for cardiac ischemia, but "for completion, check troponin and ECG." Vasospastic angina is commonly the worst in the morning and at night.
Given the consistency of the clinical profile with typical angina, associated risk factors, and abnormal ECG findings, a cardiology consult was promptly requested. It should be known that each category can easily manifest the generic subendocardial ischemia pattern. What’s interesting is that the ECG can only detect ischemia.
Whether stenting a narrowed coronary artery improves symptoms such as chest pain (angina) or shortness of breath is a very different question. Share Angina The classic definition of angina involves the sensation of tightness in the centre of the chest that is brought on with exertion and is relieved with rest. The result?
This proves effective treatment of the recurrent ischemia. The patient had no further symptoms of ischemia. Learning Points: Type 1 MI is the type we are most familiar with: rupture of atherosclerotic plaque with production thrombus or platelet fibrin aggregates. This proves effective treatment of the recurrent ischemia."
Smith comment: T-wave inversion such as seen in the first ECG can be seen with active non-transmural ischemia. But in this case, it is due to active ischemia, resolves with resolution of ischemia, and has little if any troponin elevation. Unstable Angina still exists. Thus, unstable angina exists and can be deadly.
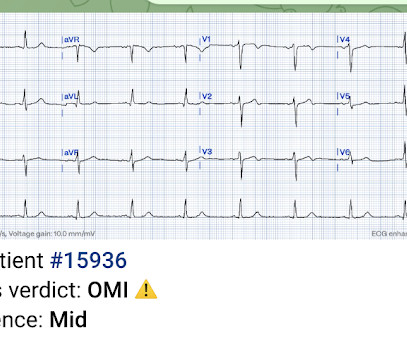
The baseline ECG is basically normal with no ischemia. You can see in the lead-specific analysis that she "sees" the STD in V5, V5, and II, with STE in aVR as signs of "Not OMI", because subendocardial ischemia pattern is not the same as OMI. In my opinion, I think it looks more like subendocardial ischemia. As per Drs.
This was diagnosed by IVUS (intravascular ultrasound) as a ruptured plaque. This was clearly severe subepicardial ischemia causing ST Elevation, but it was not of a long enough duration to result in measurable infarct. Therefore this is " Transient ST Elevation Unstable Angina." Values: STE60V3 = 2.0, QRS V2 = 10, RAV4 = 15.5,
For example, if a coronary artery becomes blocked due to plaque buildup (a condition known as coronary artery disease), the heart muscle may not receive enough oxygen, leading to chest pain (angina) or, in more severe cases, a heart attack. CAD is one of the leading causes of heart attacks.
Atherosclerotic cardiovascular disease (ASCVD), caused by plaque buildup in arterial walls, is one of the leading causes of disability and death worldwide.1,2 7 Research has shown inflammation plays a significant role in the development of atherosclerosis and ASCVD,8-10 and even the formation of plaque.11 4 In the U.S.
ET Main Tent (Hall B1) This session offers more insights from key clinical trials presented at ACC.24 24 and find out what it all means for your patients.
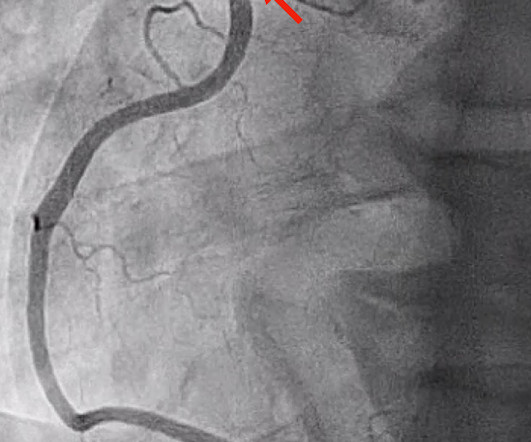
Takotsubo is a sudden event, not one with crescendo angina. To prove there is no plaque rupture, you need to do intravascular ultrasound (IVUS). An angiogram is a "lumenogram;" most plaque is EXTRALUMINAL!! I need to innoculate you against the subsequent opinions below. It can only be seen by IVUS. MINOCA has many etiologies.
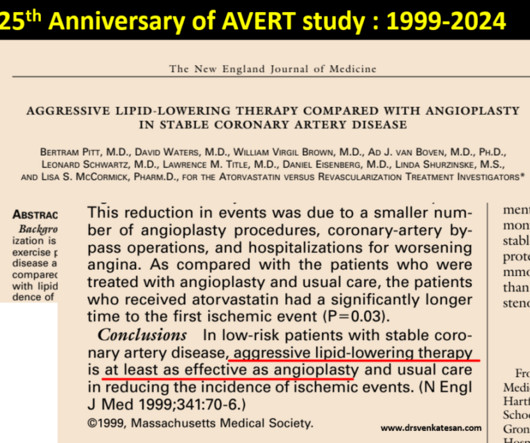
This study tested PTCA vs with a single lipid lowering drug in terms of plaque regression. Bertram Pitt and his team scripted this from the Department of Medicine, University of Michigan School of Medicine, Ann Arbor, USA. One can’t expect even in your dreams a study like this would be be done in the future.
Session 510) To Treat or Not to Treat Anatomy and Ischemia? (Session 508) Battle of the Imagers - Jeopardy Edition! Session 509) Who Wants to Be a Millionaire in Eradicating Vascular Medicine Disparities?
Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. It they are static, then they are not due to ischemia. This is better evidence for ischemia than any other data point. Again, cath lab was not activated. What does this troponin level mean? Int J Cardiol.
There is low voltage in the precordium which always makes reading ischemia harder. In ACS, chest pain is the warning sign of ongoing ischemia. Smith : As Willy says, and as we've said many times before, morphine will resolve pain without resolving ischemia. ECG 1 What do you think? To me, this ECG is not diagnostic.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content