This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In the ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) trial, researchers examined the risk of ischemic events in patients with stable coronary artery disease. years, with 57.1% occurring within 30 days after CABG. Original article: Redfors B et al.
This confirms that the pain was ischemia and is now resovled. Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardialinfarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque. The i nitial hs troponin I returned 75%.
Myocardialischemia may induce myocardial fibrosis, a condition that progressively leads to ventricular remodeling, heightening the risk of heart failure. The timely detection of myocardial fibrosis is crucial for intervention and improved outcomes. The results demonstrated tracer-specific uptake (SUVmax = 4.6)
This EKG is diagnostic of transmural ischemia of the inferior wall. Smith: note also the terminal QRS distortion in lead III (absence of S-wave without a prominent J-wave). . __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand).
The impact of this narrowing can ultimately result in angina (chest pain), which has been shown to double the risk of major cardiovascular events,1 as well as myocardialinfarction ( heart attack ) or even death. Use Heart to Act on Angina. Available at: [link]. Accessed May 2024.
By definition , this is acute myocardialinfarction, the only question now is the etiology. It is not clear exactly what symptoms the patient may have been experiencing at this time, but the notes indicate that he then developed "worsening" pain, suggesting he had likely had ongoing angina the whole time.
For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. In this case, the duration of ischemia was so brief that there was no such evolution, and there was near-normalization. Wellens' syndrome represents a state of reperfusion of the infarct related artery 2. Lessons: 1.
Although radiation into the left arm is most classic for coronary ischemia, radiation into both arms is actually modestly more predictive ). The primary care physician's note indicates low suspicion for cardiac ischemia, but "for completion, check troponin and ECG." Vasospastic angina is commonly the worst in the morning and at night.
This is a value typical for a large subacute MI, n ormal value 48 hours after myocardialinfarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). Mechanical complications secondary to myocardialinfarction are infrequent due to most patients receiving revascularization quite rapidly.
ET Main Tent (Hall B1) This session offers more insights from key clinical trials presented at ACC.24 24 and find out what it all means for your patients.
The patient was given aspirin, heparin, morphine, and ondansetron and and transferred to a PCI-capable facility for a diagnosis of "unstable angina" with dynamic ECG changes. AIVR is not always the result of significant pathology, but is classically associated with the reperfusion phase of acute myocardialinfarction.
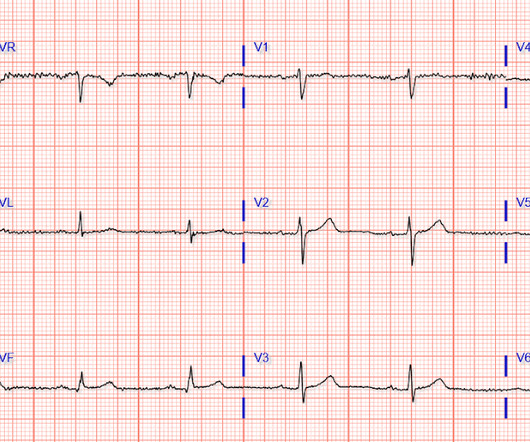
The baseline ECG is basically normal with no ischemia. You can see in the lead-specific analysis that she "sees" the STD in V5, V5, and II, with STE in aVR as signs of "Not OMI", because subendocardial ischemia pattern is not the same as OMI. In my opinion, I think it looks more like subendocardial ischemia. Eur J Emerg Med.
Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1] 1] European guidelines add "regardless of biomarkers". But only 6.4% Clin Cardiol 2022 4. Herman, Meyers, Smith et al. McLaren and Smith.
The ECG in the chart was read as "no obvious ST changes," (even though no previous ECG was available) and the formal read by the emergency physicians was: "ST deviation and moderated T-wave abnormality, consider lateral ischemia." Consequences of reocclusion after successful reperfusion therapy in acute myocardialinfarction.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
Background:Stress testing is a well-established non-invasive method commonly used in clinical practice for patients with angina. 12.8%; p<0.01; (figure 1A), ischemia was found in 36.5% (95% CI; range 28.7-44.3%; Circulation, Volume 150, Issue Suppl_1 , Page A4146032-A4146032, November 12, 2024. Follow-up ranged from 1 to 5.2
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" That said, complete LM occlusion would be expected to have subepicardial ischemia (STE) in these myocardial territories: STE vector 1.
A middle-aged woman had intermittent angina for 48 hours, then onset of constant, crushing chest pain for 1.5 Appearance of abnormal Q waves early in the course of acute myocardialinfarction: implications for efficacy of thrombolytic therapy. hours when she called 911. These do NOT indicate late, subacute MI. Raitt MH, et al.
Therefore, this does not meet the definition of myocardialinfarction ( 4th Universal Definition of MI ), which requires at least one troponin above the 99% reference range. This was clearly severe subepicardial ischemia causing ST Elevation, but it was not of a long enough duration to result in measurable infarct.
Without oxygen, the cells would quickly die, leading to a heart attack (myocardialinfarction). For example, if a coronary artery becomes blocked due to plaque buildup (a condition known as coronary artery disease), the heart muscle may not receive enough oxygen, leading to chest pain (angina) or, in more severe cases, a heart attack.
ST-elevation myocardialinfarction after pharmacologic persantine stress test in a patient with Wellens’ syndrome. Single High-Sensitivity Cardiac Troponin I to Rule Out Acute MyocardialInfarction. Evaluating Rapid Rule-out of Acute MyocardialInfarction Using a High-Sensitivity Cardiac Troponin I Assay at Presentation.
3 Patients with ASCVD are at a higher risk for major adverse cardiovascular events (MACE) including heart attack or myocardialinfarction (MI), stroke, and cardiovascular (CV) death.4 The benefit was most significant in reducing the incidence of stroke and angina requiring revascularization.35 4 In the U.S. 12 Colchicine, 0.5
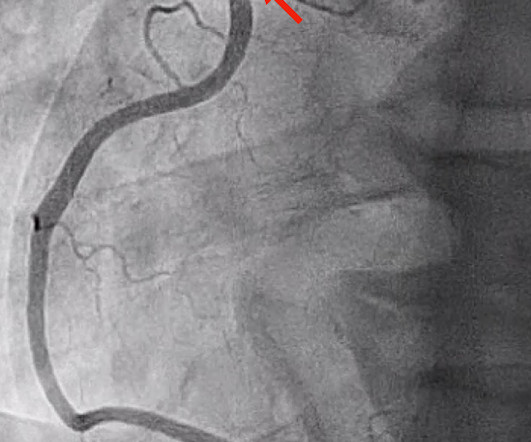
She requires maximal medical management per all current guidelines (including heparin and P2Y12 inhibitor per cardiology), as well as consideration for emergent cath in the case of persistent ischemia. So what will you do for this patient? They found an acute, total, thrombotic occlusion of the proximal LAD. They opened it. Patel et al.,
ST segment elevation in aVR in proximal LAD occlusion before first septal is thought to be due to transmural ischemia of the basal part of the septum. This patient had reported with recent onset angina. They can present with anterior wall infarction. In that case there was ST depression in I, aVL, II, aVF and V2-V6.
This is diagnostic of myocardialinfarction. Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. It they are static, then they are not due to ischemia. This is better evidence for ischemia than any other data point.
Typical angina was defined as a symptom complex that includes substernal chest pressure or pain that was made worse with exertion/emotional stress, and relieved by rest or nitroglycerin. Atypical angina is classified as having any two of the three symptoms, and non-anginal pain any one of the three symptoms. This happens. But its rare!
Takotsubo is a sudden event, not one with crescendo angina. Such cases are classified as MINOCA (MyocardialInfarction with Non-Obstructed Coronary Arteries). I need to innoculate you against the subsequent opinions below. by making it clear to everyone that this is NOT an EKG that one sees with takotsubo cardiomyopathy.
This confirms that there were dynamic signs of ischemia on the initial ECG. ng/ml , a three-fold increase from troponin #2, also confirming acute myocardialinfarction. This is particularly unusual, as T-wave normalization is usually unstable angina (negative troponin). The ST depression in aVL is also resolved.
In the STEMI/NSTEMI dichotomy, NSTEMI is supposed to mean non-occlusive myocardialinfarction, but this patient had transient Occlusion MI that was at risk for re-occlusion (like ‘transient STEMI’). Impact of total occluson of culprit artery in acute non-ST elevation myocardialinfarction: a systemic review and meta-analysis.
The highly impactful International Study of Comparative Health Effectiveness With Medical and Invasive Approaches ( ISCHEMIA ) trial investigated the effectiveness of invasive (INV) versus conservative (CON) strategies for managing stable coronary artery disease. EuroIntervention. 2024 Mar 5:EIJ-D-24-00011.
We evaluated the primary outcome (cardiovascular death, myocardialinfarction, or hospitalization for unstable angina, heart failure, or resuscitated cardiac arrest) and other end points, by sex, in 1168 (22.6%) women and 4011 (77.4%) men. of invasive‐assigned women revascularized versus 81.2%
Major findings from the INTERHEART study reveal that stress is more common among cases of acute myocardialinfarction (AMI) compared to controls. Results revealed that women are twice as likely to exhibit myocardialischemia in response to mental stress compared to traditional stressors like exercise or pharmacologic stress.
The patient might be having cardiac ischemia, but if he is, it is unstable angina or non-STEMI, or perhaps he has not YET pseudonormalized, so serial ECGs may be important. Differential of peri-infarct pericardial fluid The differential includes 1) pericarditis with effusion or 2) hemopericardium.
It could also, given a different clinical context be compatible with a subacute myocardialinfarction complicated by post infarct regional pericarditis. Due to the atypical and vague symptoms, the myocardialinfarct was not initially diagnosed. At presentation he had a history of dyspnea for 6 days.
Watch what happends as the heart recovers from its episode of ischemia. This is the c ulprit for the patient's non-ST elevation myocardialinfarction AV groove circumflex, proximal LPDA, and mid LAD stenoses may also be hemodynamically significant Occlusion of the proximal nondominant RCA is not likely clinically relevant.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content