This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Ischemia with no obstructive coronary arteries (INOCA) is an increasingly recognized condition in patients presenting with angina and positive stress tests but without significant coronary artery stenosis.
a developer of cellular and cell-derived therapeutics for the treatment of cardiovascular and pulmonary diseases, today announced the primary endpoint results of the open label roll-in cohort of the CardiAMP Cell Therapy in Chronic Myocardial Ischemia Trial. Getty Images milla1cf Thu, 05/02/2024 - 10:12 May 2, 2024 — BioCardia, Inc. ,
The perplexing landscape of angina with nonobstructive coronary arteries (ANOCA) encompasses diverse pathophysiological entities, including coronary microvascular disease (CMD), coronary artery spasm, and the enigmatic myocardial bridging (MB). Original article: Sinha A et al. Circ Cardiovasc Interv.
In the ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) trial, researchers examined the risk of ischemic events in patients with stable coronary artery disease. years, with 57.1% occurring within 30 days after CABG. Original article: Redfors B et al.
Myocardial ischemia may induce myocardial fibrosis, a condition that progressively leads to ventricular remodeling, heightening the risk of heart failure. 68 Ga-FAPI-04 PET/CT shows promise in assessing fibroblast activation in patients with early myocardial infarction characterized by prolonged myocardial ischemia.
This confirms that the pain was ischemia and is now resovled. The cardiology fellow agreed with plan for emergent cath and escorted the patient to the cath lab. Another ECG was recorded after the nitroglycerine and now without pain: All findings are resolved. The i nitial hs troponin I returned 75%.
The ORBITA-2 trial ( NCT03742050 ) investigated the efficacy of Percutaneous Coronary Intervention (PCI) compared to placebo in 301 patients with stable angina. Results revealed ischemia in one cardiac territory in 80% of patients, two territories in 17%, and three territories in 2%. compared to the placebo group (5.6; N Engl J Med.
Background Refractory angina (RA) is a chronic condition characterized by the presence of debilitating angina symptoms due to established reversible ischemia in the presence of obstructive coronary artery disease (CAD).
The ORBITA-2 (Objective Randomized Blinded Investigation With Optimal Medical Therapy of Angioplasty in Stable Angina) trial data demonstrate that, in patients with stable angina and ischemia producing coronary stenoses.
On occasion, unstable angina can present with reversible T-wave inversion during pain. When the ischemia is resolved, if there is no infarction, the T-wave can normalize. Unstable angina in the era of hs trop still exists. I know of no data on unstable angina/30-day adverse events/acute MI after 2 serial undetectable trops.
After a series of experiments in animals and peripheral vessels, he proved with a single patient N-1 study that effectively treated refractory LAD angina in a 38-year-old man in 1977. No one has questioned the efficacy of PCI for true angina with a critical lesion. Within a span of five to ten years, the concept spread globally.
In a randomized trial of PCI in patients with stable angina who were receiving little or no antianginal medication and had documented ischemia, PCI resulted in a better health status with respect to angina than placebo at 12 weeks.
The goal of the ORBITA-COSMIC trial was to determine the effects of a coronary sinus reducer (CSR) device versus sham control on both myocardial blood flow (MBF) assessed by stress perfusion cardiac magnetic resonance imaging (CMR) and daily angina burden in patients with refractory angina.
This EKG is diagnostic of transmural ischemia of the inferior wall. If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia. Transmural ischemia (as seen with the OMI findings on ECG) is not very common with demand ischemia, but is possible.
The benefit of an invasive strategy on Seattle Angina Questionnaire angina frequency scores was reduced for asymptomatic patients (odds ratio [95% credible interval], 1.16 [0.661.71] versus 2.26 [1.752.80]), as well as for those on no antianginal medications. Diabetes was present in 28% and multivessel disease in 51%.
It is not clear exactly what symptoms the patient may have been experiencing at this time, but the notes indicate that he then developed "worsening" pain, suggesting he had likely had ongoing angina the whole time. Recall that medically refractory angina is itself a Class I indication for immediate angiography (see Figure 8). (It
We sought to determine the substrates for ischemia in patients with angina, nonobstructive coronary arteries (ANOCA) and a MB in the left anterior descending artery.Methods:Patients with ANOCA underwent acquisition of intracoronary pressure and flow during rest, supine bicycle exercise and adenosine infusion.
Although radiation into the left arm is most classic for coronary ischemia, radiation into both arms is actually modestly more predictive ). The primary care physician's note indicates low suspicion for cardiac ischemia, but "for completion, check troponin and ECG." Vasospastic angina is commonly the worst in the morning and at night.
1 Indeed, if the recently published ORBITA-2 trial demonstrated the benefit of revascularisation in relieving angina symptoms, 2 many other trials aiming to show a benefit on hard outcomes have failed in their purpose. 3 The ISCHEMIA-EXTEND reported the extended follow-up of the recent ISCHEMIA trial.
The impact of this narrowing can ultimately result in angina (chest pain), which has been shown to double the risk of major cardiovascular events,1 as well as myocardial infarction ( heart attack ) or even death. Use Heart to Act on Angina. For more information: www.gehealthcare.com References: 1 World Health Federation.
Given the consistency of the clinical profile with typical angina, associated risk factors, and abnormal ECG findings, a cardiology consult was promptly requested. It should be known that each category can easily manifest the generic subendocardial ischemia pattern. What’s interesting is that the ECG can only detect ischemia.
Whether stenting a narrowed coronary artery improves symptoms such as chest pain (angina) or shortness of breath is a very different question. Share Angina The classic definition of angina involves the sensation of tightness in the centre of the chest that is brought on with exertion and is relieved with rest. The result?
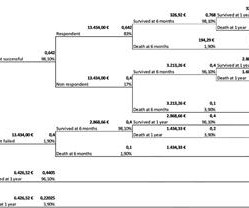
ObjectiveA significant proportion (85%) of low-risk non-ST-elevation acute coronary syndrome (NSTE-ACS) patients do not receive objective confirmation of ischemia by stress echocardiography (SE), yet remain a healthcare burden due to lower long-term survival and overuse of medical services.
This appears to be a classic Wellens' ECG, Pattern A, with terminal T-wave inversion in V2-V4, preserved R-waves, and it appears to be Wellens' syndrome, as it occurred after resolution of typical angina pain. When this happens, troponins are negative, there is no wall motion abnormality, and it is true unstable angina.
For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. In this case, the duration of ischemia was so brief that there was no such evolution, and there was near-normalization. Ischemia may be so brief that Wellens' waves do not evolve 3. The peak troponin I was 0.364 ng/ml.
Smith comment: T-wave inversion such as seen in the first ECG can be seen with active non-transmural ischemia. But in this case, it is due to active ischemia, resolves with resolution of ischemia, and has little if any troponin elevation. Unstable Angina still exists. Thus, unstable angina exists and can be deadly.
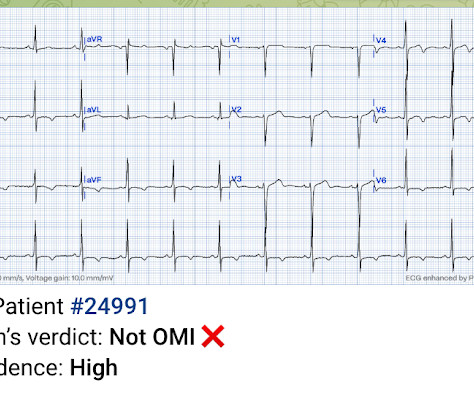
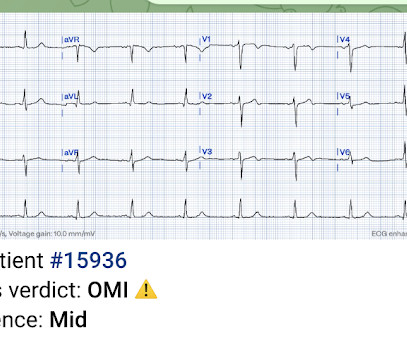
The baseline ECG is basically normal with no ischemia. You can see in the lead-specific analysis that she "sees" the STD in V5, V5, and II, with STE in aVR as signs of "Not OMI", because subendocardial ischemia pattern is not the same as OMI. In my opinion, I think it looks more like subendocardial ischemia. As per Drs.
This proves effective treatment of the recurrent ischemia. The patient had no further symptoms of ischemia. Serial EKG is very high yield diagnostic test in patients with stuttering angina. EKG 3 is diagnostic for developing re-occlusion, and EKG 4 proves that the nitrates relieved the ischemia. =
The ECG in the chart was read as "no obvious ST changes," (even though no previous ECG was available) and the formal read by the emergency physicians was: "ST deviation and moderated T-wave abnormality, consider lateral ischemia." When the ischemia is resolved, the wall motion may completely recover, or there may be persistent stunning.
Background:Stress testing is a well-established non-invasive method commonly used in clinical practice for patients with angina. 12.8%; p<0.01; (figure 1A), ischemia was found in 36.5% (95% CI; range 28.7-44.3%; Circulation, Volume 150, Issue Suppl_1 , Page A4146032-A4146032, November 12, 2024. Follow-up ranged from 1 to 5.2
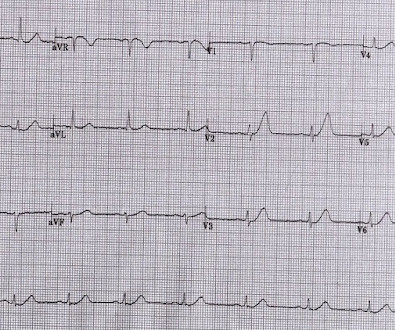
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
Non-STEMI guidelines call for “urgent/immediate invasive strategy is indicated in patients with NSTE-ACS who have refractory angina or hemodynamic or electrical instability,” regardless of ECG findings.[1] 1] European guidelines add "regardless of biomarkers". But only 6.4%
This was clearly severe subepicardial ischemia causing ST Elevation, but it was not of a long enough duration to result in measurable infarct. Therefore this is " Transient ST Elevation Unstable Angina." As there was ruptured plaque, this is NOT Prinzmetal's angina. You can see the deficiency of the definition of MI.
We are told that the Stress Echo that was performed showed objective evidence of inducible ischemia ( confirmed apparently by both wall motion abnormalities and ECG changes ). Was this objective evidence of inducible ischemia accompanied by chest pain? Was this objective evidence of inducible ischemia accompanied by chest pain?
Some persistently denied that the T-wave in V2 was a specific sign of ischemia. 2 or 3 do not rule out unstable angina, even in the era of high sensitivity troponin: this study by Thelin et al. These are 10 cases of LAD occlusion with subtle Hyperacute T-waves in lead V2 (or V3) only. Steps to verify LAD occlusion, or exclude it: 1.
The patient was given aspirin, heparin, morphine, and ondansetron and and transferred to a PCI-capable facility for a diagnosis of "unstable angina" with dynamic ECG changes. Possible mechanisms of ventricular arrhythmias elicited by ischemia followed by reperfusion. And is there new left bundle branch block (LBBB)? Moffat, M.
Because previous ischemia induces myocardial preconditioning, decreasing the likelihood of transmural myocardial necrosis and myocardial rupture, patients with evidence of diabetes mellitus, chronic angina or previous MI are less likely to experience a rupture.
Post by Smith and Meyers Sam Ghali ( [link] ) just asked me (Smith): "Steve, do left main coronary artery *occlusions* (actual ones with transmural ischemia) have ST Depression or ST Elevation in aVR?" That said, complete LM occlusion would be expected to have subepicardial ischemia (STE) in these myocardial territories: STE vector 1.
For example, if a coronary artery becomes blocked due to plaque buildup (a condition known as coronary artery disease), the heart muscle may not receive enough oxygen, leading to chest pain (angina) or, in more severe cases, a heart attack. CAD is one of the leading causes of heart attacks.
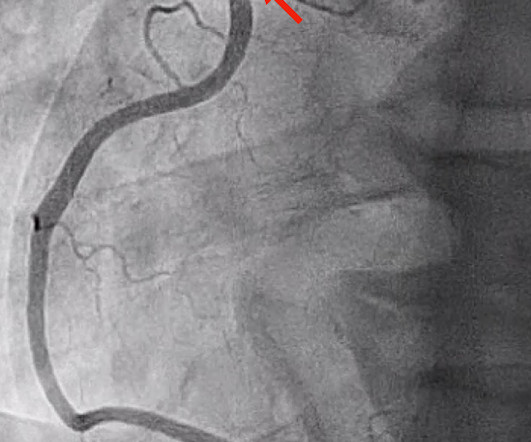
She requires maximal medical management per all current guidelines (including heparin and P2Y12 inhibitor per cardiology), as well as consideration for emergent cath in the case of persistent ischemia. So what will you do for this patient? They found an acute, total, thrombotic occlusion of the proximal LAD. They opened it. Patel et al.,
ET Main Tent (Hall B1) This session offers more insights from key clinical trials presented at ACC.24 24 and find out what it all means for your patients.
ST segment elevation in aVR in proximal LAD occlusion before first septal is thought to be due to transmural ischemia of the basal part of the septum. This patient had reported with recent onset angina. Injury current of basal part of septum is directed towards right shoulder and aVR. ST elevation was 2 mm in aVR and 1 mm in V1.
Typical angina was defined as a symptom complex that includes substernal chest pressure or pain that was made worse with exertion/emotional stress, and relieved by rest or nitroglycerin. Atypical angina is classified as having any two of the three symptoms, and non-anginal pain any one of the three symptoms. This happens. But its rare!
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.








































Let's personalize your content