This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chest pain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
Written by Willy Frick A man in his early 40s with BMI 36, hypertension, and a 30 pack-year smoking history presented with three days of chest pain. Recall that medically refractory angina is itself a Class I indication for immediate angiography (see Figure 8). (It This is WHY refractory angina should prompt immediate angiography.
ObjectiveA significant proportion (85%) of low-risk non-ST-elevation acute coronary syndrome (NSTE-ACS) patients do not receive objective confirmation of ischemia by stress echocardiography (SE), yet remain a healthcare burden due to lower long-term survival and overuse of medical services.
Given the consistency of the clinical profile with typical angina, associated risk factors, and abnormal ECG findings, a cardiology consult was promptly requested. It should be known that each category can easily manifest the generic subendocardial ischemia pattern. What’s interesting is that the ECG can only detect ischemia.
He had a history of hypertension but stopped taking his medication several years ago. This appears to be a classic Wellens' ECG, Pattern A, with terminal T-wave inversion in V2-V4, preserved R-waves, and it appears to be Wellens' syndrome, as it occurred after resolution of typical angina pain. Unstable Angina still exists 2.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chest pain relieved by rest. The baseline ECG is basically normal with no ischemia. In my opinion, I think it looks more like subendocardial ischemia.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. Also see this incredible case of the use of 12-lead ST Segment monitoring.
A VSR is more likely to occur in patients who are older, female, hypertensive, have chronic kidney disease, and have no prior history of smoking. It commonly occurs in the setting of a first myocardial infarction (MI) in the background of delayed or absent reperfusion therapy.
ET Main Tent (Hall B1) Effect of Gamification, Financial Incentives or Both Combined to Increase Physical Activity Among Patients with Elevated Risk For Major Adverse Cardiovascular Events. ET Main Tent (Hall B1) This session offers more insights from key clinical trials presented at ACC.24 24 and find out what it all means for your patients.
The patient did not report angina with stress. This ST-T wave appearance in the lateral chest leads of ECG #2 is consistent with L V “ S train” vs ischemia. No wall motion abnormality with stress. Next day, a stress echo was done: The exercise stress echocardiogram is normal. The stress electrocardiogram is non-diagnostic.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chest pain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chest pain. Takotsubo is a sudden event, not one with crescendo angina. Learning Points: 1.
In MSIMI (Mental Stress-induced Myocardial Ischemia) studies , mental stress activities like public speaking were evaluated for their impact on ischemia, measured via myocardial SPECT and vascular function (microvascular function, endothelial function). Combining behavioral and pharmacological treatment is most effective.
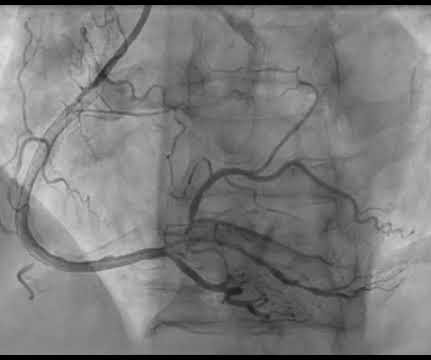
A middle-aged woman with history of hypertension presented to another hospital approximately 2 hours after onset of chest pain and shortness of breath. Back to the case: The providers recognized persistent ischemia and likely occlusion, and discussed this with cardiology who took the patient immediately for cath. mm STE in V1 and 1.5-2.0
Typical angina was defined as a symptom complex that includes substernal chest pressure or pain that was made worse with exertion/emotional stress, and relieved by rest or nitroglycerin. Atypical angina is classified as having any two of the three symptoms, and non-anginal pain any one of the three symptoms. years of age versus 59.0±8.4
Written by Willy Frick A man in his 60s with hypertension and prior stroke presented with three days of crushing chest pain. Unfortunately, although natively conducted beats are the best ones for evaluating ischemia, we only have a few! Moving on to ischemia , the ECG shows reperfused inferoposterolateral infarct.
Denying patients the potential benefit of revascularization just because their symptoms have lasted a certain amount of time shows poor understanding of the pathophysiology of myocardial ischemia. There were no other causes of dyspnea apparent and thus we can assume that myocardial ischemia started 6 days prior.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





















Let's personalize your content