This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
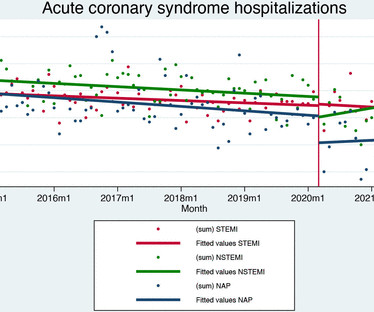
Aims We evaluated the effects of the COVID-19 pandemic on hospital admission and quality of care for acute coronary syndrome. Data on 21 001 patients were included (7057 ST-elevation myocardialinfarction (STEMI), 7649 non-ST elevation myocardialinfarction (NSTEMI) and 6295 unstable angina).
Abstract Aim Sense of coherence (SOC) allows individuals to be more resilient to adverse life events and it is associated with quality of life (QoL), but its long-term effects are unknown in patients with myocardialinfarction. Data were analysed with repeated measure ANOVA and linear regression.
She presented to an outside hospital after several days of malaise and feeling unwell. This is a value typical for a large subacute MI, n ormal value 48 hours after myocardialinfarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). At the time of admission, her vital signs were normal. Hammill SC.
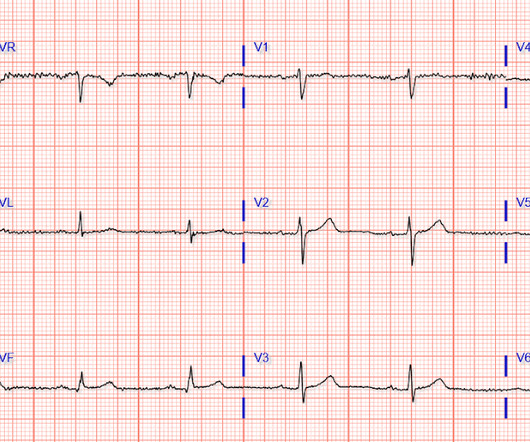
Patient is pain free and clearly has Wellens' syndrome: 1) pain free episode following an episode of angina, typical Pattern A (biphasic, terminal T-wave inversion with an initial upsloping ST Segment) findings, preserved R-waves. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction.
A middle-aged man complained of 15 minutes of classic angina that resolved upon arrival to the ED. So this is indeed diagnostic of myocardialinfarction. Not immediately, at least, because this is NOT diagnostic of ACUTE (occlusion) myocardialinfarction (Acute OMI). Here is his initial ECG: What do you think?
Answer: This is MINOCA -- MyocardialInfarction with Non-Obstructive Coronary Arteries. Comprehensive coronary evaluation (with testing for vasospasm and microvascular dysfunction) was shown in the randomized trial CorMicA to significantly improve angina, quality of life, and diagnostic accuracy. The name is self-explanatory.
Primary outcomes were all-cause, cardiovascular and non-cardiovascular mortality either in-hospital or at 1, 3 and 5 years postdischarge. Hazards of myocardialinfarction and readmission for angina at 1, 3 and 5 years were significantly greater for TAVR. Secondary outcomes included adverse outcomes and readmission.
The scan also showed “scattered coronary artery plaques”. __ Smith comment 1 : the appropriate management at this point is to lower the blood pressure (lower afterload, which increases myocardial oxygen demand). If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia.
We present the cumulative percutaneous coronary intervention (PCI) data of all comers (stable angina and acute coronary syndromes [ACS]) who presented to Hadi Clinic between January 2018 and December 2020. A total of 567 patients underwent coronary catheterisation for the three-year period between January 2018 and December 2020.
Prior Indications in the U.S.: To reduce the risk of myocardialinfarction, stroke, and unstable angina requiring hospitalization in adults with established cardiovascular disease.
ST-elevation myocardialinfarction after pharmacologic persantine stress test in a patient with Wellens’ syndrome. Single High-Sensitivity Cardiac Troponin I to Rule Out Acute MyocardialInfarction. Evaluating Rapid Rule-out of Acute MyocardialInfarction Using a High-Sensitivity Cardiac Troponin I Assay at Presentation.
Another ECG was recorded 5 minutes later just before arrival at the hospital: Similar The patient was transported to a nearby suburban hospital with PCI capabilities while my partner cared for her. Takotsubo is a sudden event, not one with crescendo angina. She was defibrillated and resuscitated. It can only be seen by IVUS.
Post by Smith, with short article by Angie Lobo ( [link] ), a third year intermal medicine resident at Abbott Northwestern Hospital Case A 30-something woman with no past history, who is very fit and athletic, presented with 1.5 It was late evening and the patient will be in the hospital overnight with a potentially very unstable LAD lesion.
The term MINOCA stands for Myocardialinfarction with non-obstructive coronary arteries. A 50-year-old lady was admitted to my hospital with crushing chest tightness. I’ll try and explain this a bit better by using a case study. She had an ECG which suggested changes in keeping with a lack of blood getting to the heart.
ng/ml , a three-fold increase from troponin #2, also confirming acute myocardialinfarction. This is particularly unusual, as T-wave normalization is usually unstable angina (negative troponin). This confirms that there were dynamic signs of ischemia on the initial ECG. It was not normal! A third troponin I returned at 0.27
BackgroundStrain assessed by cardiac magnetic resonance (CMR) is a key prognostic indicator in myocardialinfarction. However, the strain characteristics and prognostic value in myocardialinfarction with nonobstructive coronary arteries (MINOCA) with different causes are unclear.
The study utilized the ISCHEMIA primary outcome, a composite measure of cardiovascular death, protocol-defined myocardialinfarction, or hospitalization for unstable angina, heart failure, or resuscitated cardiac arrest. years, with 57.1% occurring within 30 days after CABG.
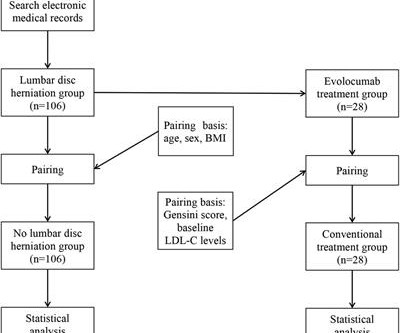
Methods In this study, a total of 212 patients (age 46–80 years) with unstable angina (UA) who underwent coronary angiography (CAG) in our hospital from January 2018 to July 2022 due to UA were included. Objective Assessing the impact of lumbar disc herniation (LDH) on the plaque burden of coronary atherosclerosis is our objective.
The primary outcome was a composite of death from any cause, myocardialinfarction, or hospitalization for unstable angina at 2 years. High-risk PCI patients were randomized to routine functional testing at 1 year or standard care alone during follow-up.
years, and low baseline prevalence of cardiovascular disease (myocardialinfarction, 5.1%; cerebrovascular accident, 2.0%) were followed for a median of 5 years. MACE outcomes and hospitalization for heart failure in the liraglutide-treated group were compared with the other groups combined using Cox proportional hazards models.
The impact of this narrowing can ultimately result in angina (chest pain), which has been shown to double the risk of major cardiovascular events,1 as well as myocardialinfarction ( heart attack ) or even death. Use Heart to Act on Angina. Available at: [link]. Accessed May 2024.
of the patients were diagnosed with non-ST elevated myocardialinfarction (NSTEMI), 36.8% with ST elevated myocardialinfarction (STEMI), 3.41% with unstable angina, 0.56% with stable angina, and 0.11% were diagnosed with various types of arrhythmias. Approximately 48.5% and 1.3%, respectively.
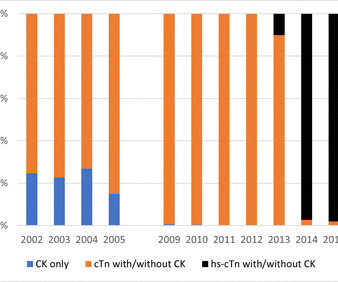
Background Since 2000, the definition of myocardialinfarction (MI) has evolved with reliance on cardiac troponin (cTn) tests. The implications of this change on trends of acute coronary syndrome (ACS) subtypes obtained from routinely collected hospital morbidity data are unclear.
Background:Continuity of care is crucial to enabling a seamless chain of care after hospitalization due to cardiac conditions. Factorial ANOVA was used to analyze interactions or main effects of sex, age (<65 or ≥65), and diagnosis (angina, atrial fibrillation, heart failure, myocardialinfarction) on perceived continuity of care.
Background On the one hand, the primary coronary slow flow phenomenon (CSFP) can cause recurrence of chest pain, prompting medical examinations and further healthcare costs, while on the other hand, it can lead to myocardialinfarction, ventricular arrhythmia and sudden cardiac death.
A middle-aged woman had intermittent angina for 48 hours, then onset of constant, crushing chest pain for 1.5 Appearance of abnormal Q waves early in the course of acute myocardialinfarction: implications for efficacy of thrombolytic therapy. hours when she called 911. These do NOT indicate late, subacute MI. Raitt MH, et al.
The overall mortality, cardiac deaths, myocardialinfarctions, and hospitalizations for unstable angina were acquired from national registry data for 1 to 10 years of follow‐up (median, 4 years). PTP was calculated according to the 2013 and 2019 ESC guidelines.
EMPACT-MI 1 ( NCT04509674 ) studied the effects of empagliflozin in patients who have experienced myocardialinfarction (MI). Investigators assessed if empagliflozin could lower the risk of hospitalization for heart failure (HF) or death from cardiovascular disease (CVD). Here is our curated list of the top sessions.
3 Patients with ASCVD are at a higher risk for major adverse cardiovascular events (MACE) including heart attack or myocardialinfarction (MI), stroke, and cardiovascular (CV) death.4 Nearly 20% of those people who have had a MI will be hospitalized again within five years due to a second event.5 4 In the U.S. N Engl J Med.
Patients with CI had a greater cumulative hazard ratio for death and hospitalizations due to myocardialinfarction or unstable angina (Image 1).Conclusion:These The Tanaka formula revealed similar results (p <0.001).Patients Conclusion:These results demonstrate that CI is linked to lower RHR.
At the bottom of the post, I have re-printed the section on aVR in my article on the ECG in ACS from the Canadian Journal of Cardiology: New Insights Into the Use of the 12-Lead Electrocardiogram for Diagnosing Acute MyocardialInfarction in the Emergency Department Case 1. Current Emergency and Hospital Medicine Reports 2013;1:43-52.
A middle-aged woman with history of hypertension presented to another hospital approximately 2 hours after onset of chest pain and shortness of breath. They collected several repeat ECGs at the outside hospital before transport: None of these three ECGs meet STEMI criteria. This ECG was recorded on arrival: What do you think?
Typical angina was defined as a symptom complex that includes substernal chest pressure or pain that was made worse with exertion/emotional stress, and relieved by rest or nitroglycerin. Atypical angina is classified as having any two of the three symptoms, and non-anginal pain any one of the three symptoms.
The TIMI (Thrombolysis in MyocardialInfarction) Study Group is a Division of Cardiovascular Medicine at the esteemed Brigham and Women’s Hospital and Harvard Medical School. Anish Koka, MD @anish_koka This was driven almost entirely by myocardialinfarction / need for revascularization.
Methods A large-scale cohort study of patients with ST-elevation/non-ST-elevation myocardialinfarction (MI)/unstable angina underwent coronary angiography (January 2015–December 2019). Older patients had a greater risk of in-hospital mortality than younger patients (adjusted OR (aOR) 2.12, 95% CI 1.62
We evaluated the primary outcome (cardiovascular death, myocardialinfarction, or hospitalization for unstable angina, heart failure, or resuscitated cardiac arrest) and other end points, by sex, in 1168 (22.6%) women and 4011 (77.4%) men. of invasive‐assigned women revascularized versus 81.2%
Even though guidelines say that patients with high-risk features, refractory angina, instability, etc. How is a patient permitted to infarct his inferior wall in a cath capable facility while being monitored for known myocardialinfarction. This is the limitation of STEMI. Less than 1 in 15 in fact.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




































Let's personalize your content