This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
(MedPage Today) -- Exercise electrocardiographic (ECG) stress tests appeared to reliably indicate that some patients with angina with nonobstructive coronary arteries (ANOCA) actually had coronary microvascular dysfunction (CMD), preliminary evidence.
The perplexing landscape of angina with nonobstructive coronary arteries (ANOCA) encompasses diverse pathophysiological entities, including coronary microvascular disease (CMD), coronary artery spasm, and the enigmatic myocardial bridging (MB). Original article: Sinha A et al. Circ Cardiovasc Interv.
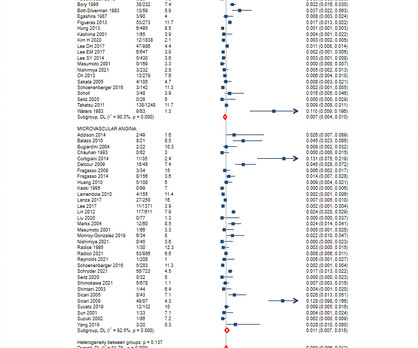
What is the specificity of exercise electrocardiogram stress testing (EST) in detecting ischemic substrate in patients with angina and nonobstructive coronary arteries (ANOCA)?
BackgroundVasospastic angina usually presents with intermittent episodes of chest pain. The patient had abnormal smell sensation and shortness of breath at the initiation of exercise stress echocardiography with transient electrocardiographic changes and new regional wall motion abnormalities.
Results from the open label roll-in cohort of patients having chronic myocardial ischemia with refractory angina showed an average increase in exercise tolerance of 107 seconds and an average of 82% reduction in angina episodes at the primary six-month follow-up endpoint compared to before receiving the study treatment.
We aimed to identify non-ischemic phenotypes in low-risk NSTE-ACS patients by analyzing a wide range of parameters available during exercise SE.MethodsInpatients [n=103, median age 56 (4665)years, 65 (63%) men] with suspected NSTE-ACS without high-risk criteria underwent exercise SE using a semi-supine cycle ergometer.
It is primarily indicated for refractory angina that is not amenable to PCI or CABG with the opinion of a cardiologist. Despite being a heart transplantation candidate, she declined revascularization and sought alternative treatments for angina, dyspnea, and daily activity limitations.
This condition reduces blood flow to the heart, increasing the risk of angina (chest pain) and heart attacks. Exercise Regularly : Aim for at least 150 minutes of moderate-intensity aerobic activity per week, such as walking, cycling, or swimming.
1 2 The exercise ECG, once the stalwart of chest pain evaluation, has lost favour over the last two decades in most heart centres due to its relatively poor discriminatory ability and reliance on patients to walk on a treadmill.
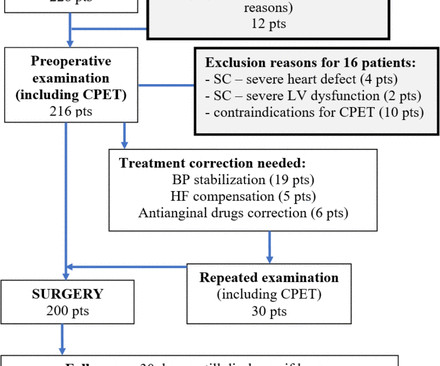
Background Cardiopulmonary exercise testing (CPET) has shown to be useful for preoperative risk stratification in various types of intra-abdominal and thoracic surgery. However, data about the predictive value of CPET for cardiovascular outcome after gastric or oesophageal cancer surgery are inconclusive. to 22.47).
The typical pain of cardiac origin is a central chest pain which occurs on walking or other forms of exercise, known as effort angina. Effort angina is commonly due to significant obstruction to a blood vessel (coronary artery) supplying a part of the heart muscle. A pain lasting more than 30 minutes is usual.
The patient was referred for an exercise nuclear study and did 11 min on the Bruce protocol without angina or ischaemic ECG changes. There was no pertinent family history. Physical examination, an ECG, basic laboratories and a chest X-ray were unremarkable. Myocardial scintigraphic perfusion images at stress and rest were normal.
Whether stenting a narrowed coronary artery improves symptoms such as chest pain (angina) or shortness of breath is a very different question. Share Angina The classic definition of angina involves the sensation of tightness in the centre of the chest that is brought on with exertion and is relieved with rest. The result?
The primary outcome was change in treadmill exercise time, and the secondary outcome was change in Seattle Angina Questionnaire summary score in response to anti-ischemic therapy. Baseline exercise time and Seattle Angina Questionnaire summary scores were similar between groups. and reference group if CFR≥2.5.
He first noticed it while exercising. Thus, the patient does not (yet) get a formal diagnosis of MI and must be called unstable angina unless further troponins return above the 99th percentile. On the basis of unresolved angina, cardiology decided to perform rescue PCI. The following ECG was obtained around midnight.
Background The prognosis of myocardial ischaemia with no obstructive coronary artery disease (INOCA) and its underlying vasomotor disorders, vasospastic angina (VSA) and microvascular angina (MVA), is not well defined. The rate of MACE with VSA was 1.1 (95% 95% CI 0.5 100 patient-years and with MVA was 2.5 (95% 95% CI 1.6 95% CI 2.0
DECISION-CTO,EURO-CTO,EXPLORE,IMPACTOR) Opening a CTO, for reasons other than angina (i.e. The role of collateral circulation in CTO that can compensate even during exercise is well known at patient level data. The normally aggressive American guidelines exercise much caution with a 2B punch. Surprise… surprise !,
Episodes of angina over past couple of months had been progressive. The fact that the 50yo man in today's case has known coronary disease ( including exercise-induced angina over the previous 3 months ) — means that even before looking at his initial ECG — statistical odds that his regular WCT rhythm will be VT are at least 90%.
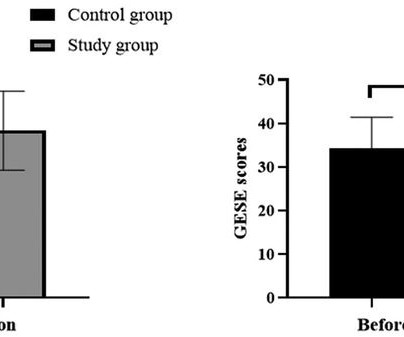
After the intervention, there was no significant change in the proportions of smokers, alcohol consumers, and individuals engaging in leisure exercises in the control group. Avoidance and surrender scores significantly increased after the intervention, with the study group scoring significantly lower than the control group.
Background:Cardiac output reserve and exercise capacity are strong predictors of life expectancy. Chronotropic incompetence (CI) is the inability to reach an age appropriate maximum heart rate with exercise. CI reduces cardiac output reserve and exercise capacity, both of which increase all-cause mortality risk. x age in years).Results:The
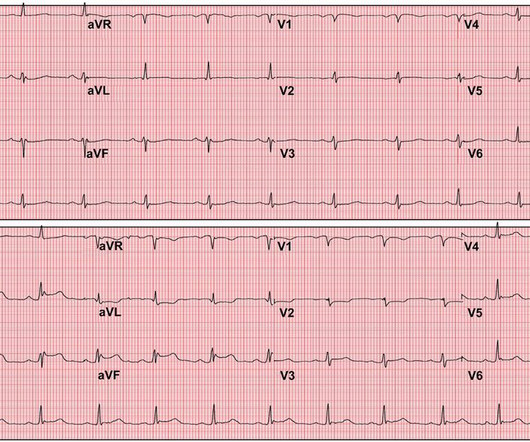
We sought to determine the substrates for ischemia in patients with angina, nonobstructive coronary arteries (ANOCA) and a MB in the left anterior descending artery.Methods:Patients with ANOCA underwent acquisition of intracoronary pressure and flow during rest, supine bicycle exercise and adenosine infusion. 0.05; CFR was 2.5±0.5,
This can lead to chest pain (angina) and increase your risk of heart attack or stroke, especially if you already have underlying heart disease. Techniques like regular exercise, deep breathing, meditation, and seeking social support can help you manage stress more effectively and mitigate its cardiovascular impacts.
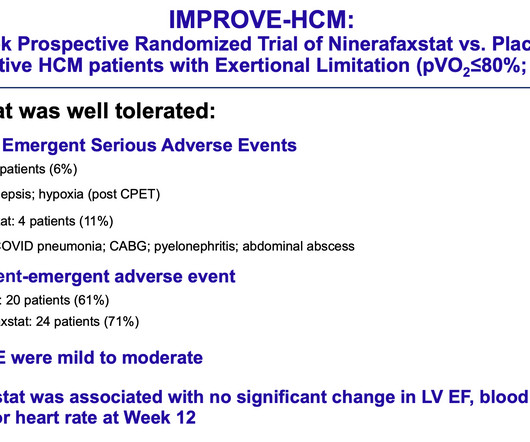
Maron, MD “Our findings provide enthusiasm that a novel drug therapy with ninerafaxstat may provide nonobstructive HCM patients an opportunity to achieve a better quality of life by decreasing symptom burden and improving exercise capacity,” said Martin S. The study was funded by Imbria Pharmaceuticals, developer of ninerafaxstat.
For example, if a coronary artery becomes blocked due to plaque buildup (a condition known as coronary artery disease), the heart muscle may not receive enough oxygen, leading to chest pain (angina) or, in more severe cases, a heart attack. CAD is one of the leading causes of heart attacks.
Among additional diagnostic tests to consider for this patient would be an Echo ( ideally performed during an episode of chest pain! ) — Cardiac MRI with LGE ( as one of the KEY tests for identifying the etiology of MINOCA in a majority of patients ) — and a simple, maximal-effort Exercise Treadmill Test ( to better evaluate the effect of this patient's (..)
ET Main Tent (Hall B1) A Selective Aldose Reductase Inhibitor (at-001) For the Treatment of Diabetic Cardiomyopathy: Primary Results of the Phase 3 Randomized Controlled ARISE-HF Study Efficacy and Safety of Ninerafaxstat, a Novel Cardiac Mitotrope, in Patients with Symptomatic Nonobstructive Hypertrophic Cardiomyopathy: Results of IMPROVE-HCM Topical (..)
If objective ECG and Echo evidence of induced ischemia occurred within the first few minutes of low-level exercise — then even IF the clinicians failed to appreciate that this patient’s initial ECG was diagnostic for a recent event — there is NO WAY this patient should have had to wait 2 weeks for an “elective angiogram”.
The problem with both these tests are that they study the heart at rest and sometimes abnormalities may be picked up only when the heart is stressed and therefore combining these modalities with a stress test can be even more helpful and by far the best form of stress is exercise.
Angina is another common symptom due the hypertrophy which causes a coronary supply demand mismatch Symptoms of HCM include syncope/near syncope, which could be precipitated by exertion, hypovolemia, rapid standing, Valsalva manoeuvre, diuretics, vasodilators or arrhythmia.
The ECG in Figure-1 was obtained from a previously healthy middle-aged man — who while performing his regular exercise routine, developed "slight" chest discomfort and "palpitations". These symptoms persisted for over an hour, which led the patient to contact EMS.
As an exercise, lets calculate the equation for differentiating the ST elevation between benign early repolarization and LAD occlusion. This transient occlusion can happen repeatedly without even making a troponin if the episodes are brief enough, and this type of stuttering event is what used to be the meaning of the term unstable angina.
Next day, a stress echo was done: The exercise stress echocardiogram is normal. The patient did not report angina with stress. No wall motion abnormality at rest. No wall motion abnormality with stress. The stress electrocardiogram is non-diagnostic.
Lifestyle Habits: Obesity, smoking, excessive alcohol consumption, and lack of exercise can all negatively impact sexual function. The aim is to restore proper blood flow to the heart, alleviating symptoms like chest pain (angina) and reducing the risk of heart attacks.
Results revealed that women are twice as likely to exhibit myocardial ischemia in response to mental stress compared to traditional stressors like exercise or pharmacologic stress. Moreover, women under 50 years old are four times more likely to experience MSIMI. Combining behavioral and pharmacological treatment is most effective.
How common is angina in DCM ? Angina in DCM is an exception despite elevated LVEDP. Is the above logic explain why very few dilated cardiomyopathy patients experience angina? Even in ischemic cardiomyopathy, once it sets in, Intensity of angina is mitigated or completley eliminated.(of of course at the cost of failure).
BackgroundPainful left bundle branch block (LBBB) syndrome is an uncommon disease that is defined as intermittent episodes of angina associated with simultaneous LBBB changes on an electrocardiogram (ECG) with the absence of flow-limiting coronary artery disease or ischemia on functional testing.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.


































Let's personalize your content