This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction.
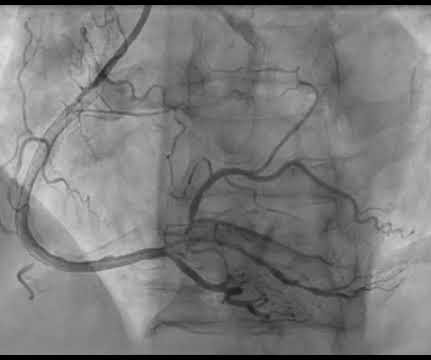
Patients with dextrocardia present a diagnostic challenge, particularly in the context of acute coronary syndrome.Case Presentation:A 49-year-old male with a medical history of dextrocardia, hypothyroidism, dyslipidemia and hypertension was referred to a cardiologist by his primary physician due to a 3-week history of unstable angina.
A stent was placed. For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. When there is extremely brief ischemia, as in this case , or this case , it may entirely reverse, especially in unstable angina (negative troponins). The peak troponin I was 0.364 ng/ml. Lessons: 1.
As hours go by, these T inversions always evolve , [unless 1) there is re-occlusion, in which case they go upright and become hyperacute, with or without additional ST elevation, ("pseudonormalize") or 2) no infarction at all (negative troponin, true unstable angina with dynamic T-waves, in which they may normalize). It was stented.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. The patient underwent successful placement of one drug eluting stent with restoration of TIMI 3 flow.
The lesion was stented. These are reperfusion T-waves (the same thing as Wellens' waves) Echocardiogram Regional wall motion abnormality-distal septum and apex. It seems that there was some uncertainly about this. Int J Cardiol. 2016;207:341–348. doi: 10.1016/j.ijcard.2016.01.188. 2016.01.188. Saw J, Mancini GBJ, Humphries KH.
Echocardiogram showed inferior wall hypokinesis. On Sunday, the patient complained of dyspnea and angina while ambulating. The second operator described the RCA as an acute thrombotic occlusion and placed three overlapping stents. Initial hsTnI was 14,114 ng/L, repeat 12,651 ng/L, none further checked. Repeat ECG is shown.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














Let's personalize your content