This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Nossen also pointed out that with voltage this high in the limb leads, you would typically expect some degree of inferior/inferolateral ST depression (the so-called "LVH strain" pattern), and in fact this patient did have severe LVH on subsequent echocardiogram (which Dr. Nossen did not know at the time). The troponin peaked at 25749 ng/L.
Given the consistency of the clinical profile with typical angina, associated risk factors, and abnormal ECG findings, a cardiology consult was promptly requested. It should be known that each category can easily manifest the generic subendocardial ischemia pattern. What’s interesting is that the ECG can only detect ischemia.
For those who depend on echocardiogram to confirm the ECG findings of ischemia, this should be sobering. In this case, the duration of ischemia was so brief that there was no such evolution, and there was near-normalization. Ischemia may be so brief that Wellens' waves do not evolve 3. The peak troponin I was 0.364 ng/ml.
The ECG in the chart was read as "no obvious ST changes," (even though no previous ECG was available) and the formal read by the emergency physicians was: "ST deviation and moderated T-wave abnormality, consider lateral ischemia." When the ischemia is resolved, the wall motion may completely recover, or there may be persistent stunning.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
When flow is restored, wall motion may completely recover so that echocardiogram does not detect the previous ischemia. Even when the serial troponins are negative, the ECG is critical to the diagnosis of ACS. This is not pericarditis because: a. Pain was typical for MI (substernal, not postional or sharp, resolved with NTG) b.
Now you have ECG and troponin evidence of ischemia, AND ventricular dysrhythmia, which means this is NOT a stable ACS. These are reperfusion T-waves (the same thing as Wellens' waves) Echocardiogram Regional wall motion abnormality-distal septum and apex. It they are static, then they are not due to ischemia. Int J Cardiol.
Next day, a stress echo was done: The exercise stress echocardiogram is normal. The patient did not report angina with stress. This ST-T wave appearance in the lateral chest leads of ECG #2 is consistent with L V “ S train” vs ischemia. No wall motion abnormality at rest. No wall motion abnormality with stress.
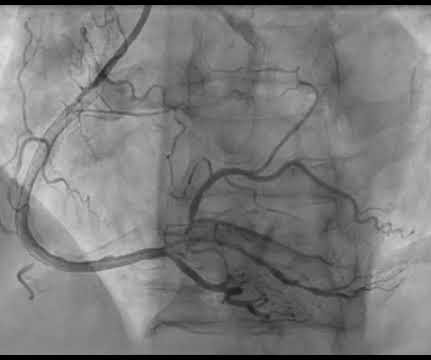
Takotsubo is a sudden event, not one with crescendo angina. Here is the cath report: Echocardiogram: There is severe hypokinesis of entire LV apex and apical segment of all the walls. An apical OMI has the same ultrasound findings as takotsubo, and thus mimics takotsubo. Learning Points: 1. Learn to Recognize Hyperacute T-waves 2.
Watch what happends as the heart recovers from its episode of ischemia. Case continued Troponins over 26 hours, from right to left : Echocardiogram: Mild concentric left ventricular wall thickening, normal cavity size, and normal systolic function. The ECG shows inferior ischemia. Are the T-waves in leads I and II hyperacute?
Unfortunately, although natively conducted beats are the best ones for evaluating ischemia, we only have a few! Moving on to ischemia , the ECG shows reperfused inferoposterolateral infarct. Echocardiogram showed inferior wall hypokinesis. On Sunday, the patient complained of dyspnea and angina while ambulating.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.

















Let's personalize your content