This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Willy Frick A man in his early 40s with BMI 36, hypertension, and a 30 pack-year smoking history presented with three days of chest pain. Recall that medically refractory angina is itself a Class I indication for immediate angiography (see Figure 8). (It This is WHY refractory angina should prompt immediate angiography.
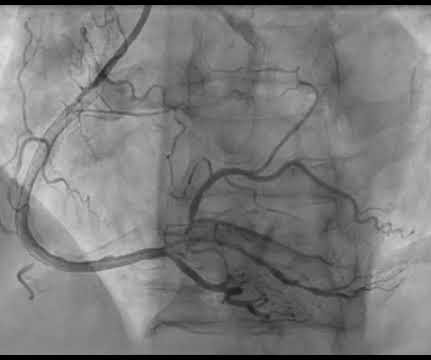
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chest pain. His echocardiogram showed normal wall motion. This is written by Willy Frick, an amazing cardiology fellow in St. Before and after of the LAD shown below.
Given the consistency of the clinical profile with typical angina, associated risk factors, and abnormal ECG findings, a cardiology consult was promptly requested. 3-vessel disease with a culprit lesion [Typical angina, multiple risk factors] b. If they all return normal, then this is unstable angina. Anemia [Normal Hgb] g.
Patients with dextrocardia present a diagnostic challenge, particularly in the context of acute coronary syndrome.Case Presentation:A 49-year-old male with a medical history of dextrocardia, hypothyroidism, dyslipidemia and hypertension was referred to a cardiologist by his primary physician due to a 3-week history of unstable angina.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chest pain, lasting 5 minutes at a time, with several episodes over the past couple of months. Also see this incredible case of the use of 12-lead ST Segment monitoring.
Angina is another common symptom due the hypertrophy which causes a coronary supply demand mismatch Symptoms of HCM include syncope/near syncope, which could be precipitated by exertion, hypovolemia, rapid standing, Valsalva manoeuvre, diuretics, vasodilators or arrhythmia. in hypertensives are some of the features.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chest pain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chest pain. Takotsubo is a sudden event, not one with crescendo angina. Learning Points: 1.
Next day, a stress echo was done: The exercise stress echocardiogram is normal. The patient did not report angina with stress. No wall motion abnormality at rest. No wall motion abnormality with stress. The stress electrocardiogram is non-diagnostic. The ST-T wave picture in lead V 3 is interesting.
Written by Willy Frick A man in his 60s with a history of hypertension and 40 pack-year history presented to the ER with 1 day of intermittent, burning substernal chest pain radiating into both arms as well as his back and jaw. Echocardiogram showed inferior hypokinesis. Troponin was rising when last checked, 8928 ng/L.
Written by Willy Frick A man in his 60s with hypertension and prior stroke presented with three days of crushing chest pain. Echocardiogram showed inferior wall hypokinesis. On Sunday, the patient complained of dyspnea and angina while ambulating. He described it as substernal with radiation into the right arm.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content