This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
In the ISCHEMIA (International Study of Comparative Health Effectiveness with Medical and Invasive Approaches) trial, researchers examined the risk of ischemic events in patients with stable coronaryarterydisease. years, with 57.1% occurring within 30 days after CABG. Original article: Redfors B et al.
The optimal surveillance strategy after percutaneous coronary intervention (PCI) for high-risk patients with multivessel or left main coronaryarterydisease (CAD) remains uncertain. The primary outcome was a composite of death from any cause, myocardial infarction, or hospitalization for unstable angina at 2 years.
Together, the two companies will work to further the development and commercialization of Medis Quantitative Flow Ratio (Medis QFR), a non-invasive approach to the assessment of coronary physiology, as part of GE HealthCare’s interventional cardiology portfolio built around the Allia Platform. Use Heart to Act on Angina.
Publication date: 15 January 2024 Source: The American Journal of Cardiology, Volume 211 Author(s): Namrita D. Ashokprabhu, Jessie Fox, Timothy D. Henry, Christian W. Schmidt, Darlene Tierney, Julie Gallatin, Yulith Roca Alvarez, Lauren Thompson, Michelle Hamstra, Sachin A. Shah, Odayme Quesada
(MedPage Today) -- ATLANTA -- For people with stable coronaryarterydisease and refractory angina, a coronary sinus reducer (CSR) implant showed a symptom alleviation benefit in the small placebo-controlled ORBITA-COSMIC trial. The number of.
Coronaryarterydisease (CAD) is frequently found in this patient group and optimal management in these patients remains uncertain. Subsidiary outcomes included patient angina and breathlessness scores. CAD at the time of TAVI also did not alter breathlessness or angina scores before/after TAVI (p>0.05).
BackgroundVasospastic angina usually presents with intermittent episodes of chest pain. Subsequent invasive coronary angiography showed no obstructive epicardial coronaryarterydisease. She reported that she often experienced an abnormal smell sensation just prior to the event.
Coronary physiology assessment, including epicardial and microvascular investigations, is a fundamental tool in the contemporary management of patients with coronaryarterydisease. Coronary revascularisation guided by functional evaluation has demonstrated superiority over angiography-only-guided treatment.
BACKGROUND:We investigated the usefulness of invasive coronary function testing to diagnose the cause of angina in patients with no obstructive coronary arteries.METHODS:Outpatients referred for coronary computed tomography angiography in 3 hospitals in the United Kingdom were prospectively screened. versus 50.9%,P<0.001).At
This quality improvement study estimates the prevalence of vasomotor dysfunction in patients with angina and no obstructive coronaryarterydisease who were clinically referred for a coronary function test; and investigates the safety and feasibility of this test in the Netherlands Registry of Invasive Coronary Vasomotor Function Testing (NL-CFT).
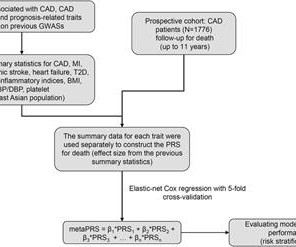
Introduction Coronaryarterydisease (CAD) is a highly heritable and multifactorial disease. Numerous genome-wide association studies (GWAS) facilitated the construction of polygenic risk scores (PRS) for predicting future incidence of CAD, however, exclusively in European populations.
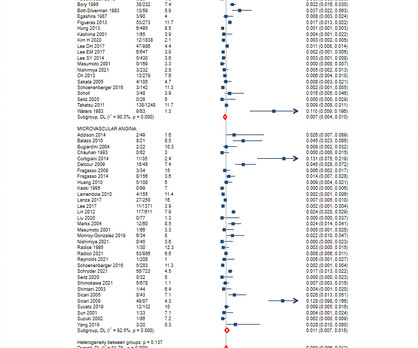
Background The prognosis of myocardial ischaemia with no obstructive coronaryarterydisease (INOCA) and its underlying vasomotor disorders, vasospastic angina (VSA) and microvascular angina (MVA), is not well defined.
Background Refractory angina (RA) is a chronic condition characterized by the presence of debilitating angina symptoms due to established reversible ischemia in the presence of obstructive coronaryarterydisease (CAD).
Background Despite tremendous therapeutic advancements, a significant proportion of coronaryarterydisease patients suffer from refractory angina pectoris, that is, quality-of-life-compromising angina that is non-manageable with established pharmacological and interventional treatment options.
Results from the open label roll-in cohort of patients having chronic myocardial ischemia with refractory angina showed an average increase in exercise tolerance of 107 seconds and an average of 82% reduction in angina episodes at the primary six-month follow-up endpoint compared to before receiving the study treatment.
Introduction Current guideline recommend functional imaging for myocardial ischaemia if coronary CT angiography (CTA) has shown coronaryarterydisease (CAD) of uncertain functional significance. However, diagnostic accuracy of selective myocardial perfusion imaging after coronary CTA is currently unclear.
Nature Reviews Cardiology, Published online: 25 April 2024; doi:10.1038/s41569-024-01033-x Findings from the ORBITA-COSMIC trial show that treatment of patients with stable coronaryarterydisease using a coronary sinus reducer improves angina symptoms but does not increase transmural myocardial perfusion.
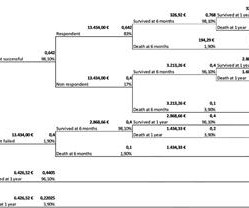
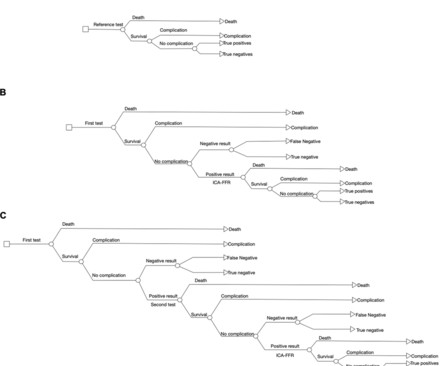
Objective Given recent data on published diagnostic accuracies, this study sought to determine the most cost-effective diagnostic strategy for detection of significant coronaryarterydisease (CAD) in stable angina patients using invasive coronary angiography (ICA) and fractional flow reserve (FFR) as the reference standard.
BackgroundCoronary computed tomography angiography is increasingly used as the first‐line test for suspected coronaryarterydisease. The overall mortality, cardiac deaths, myocardial infarctions, and hospitalizations for unstable angina were acquired from national registry data for 1 to 10 years of follow‐up (median, 4 years).
BACKGROUND:The underlying mechanisms responsible for the clinical benefits following coronary sinus narrowing and pressure elevation remain unclear. Secondary end points included changes in coronary flow reserve and the resistive resistance ratio values.
CoronaryArteryDisease (CAD) : High blood pressure accelerates the development of CAD by promoting the buildup of plaques in the coronaryarteries. This condition reduces blood flow to the heart, increasing the risk of angina (chest pain) and heart attacks.
Coronaryarterydisease (CAD) is the most common type of heart disease and the leading cause of death globally: one in four people lose their lives to CAD annually. Coronaryarteries provide the heart with the oxygen-rich blood that it needs to function, carrying away oxygen-depleted blood.
Objectives There are few reports regarding the prognosis in patients with obstructive coronaryarterydisease (OCAD) and vasospastic angina (VSA). This study investigated the clinical characteristics and clinical outcomes in patients with VSA and OCAD, especially regarding provoked spasm phenotypes and sites.
Atherosclerotic cardiovascular disease (ASCVD), caused by plaque buildup in arterial walls, is one of the leading causes of disability and death worldwide.1,2 1,2 ASCVD causes or contributes to conditions that include coronaryarterydisease (CAD), cerebrovascular disease, and peripheral vascular disease (inclusive of aortic aneurysm).3
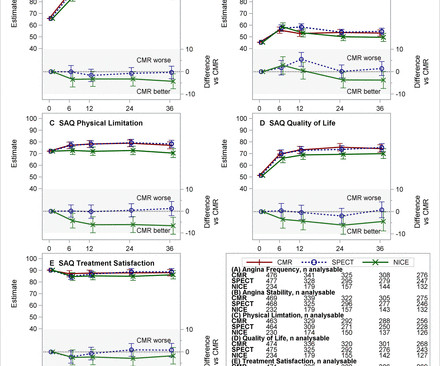
We aimed to determine whether different strategies to manage suspected stable angina affected medium-term cardiovascular event rates and patient-reported quality of life (QoL) measures. 12) Questionnaire and EuroQol-5 Dimension Questionnaire were recorded.
Subscribe now Stenting stable coronaryarterydisease has not been convincingly proven to reduce the risk of future heart attacks or death 1. Whether stenting a narrowed coronaryartery improves symptoms such as chest pain (angina) or shortness of breath is a very different question. What About Symptoms?
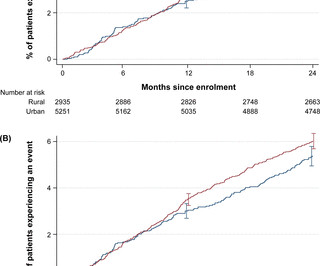
The incidence of clinical endpoints (cardiovascular (CV) death, AMI, unstable angina with urgent revascularisation and stroke; bleeding; and all-cause mortality) was analysed. Data were collected at baseline and every 6 months for 24 months. to 1.00, p=0.04); ERR=0.84 (95% CI, 0.78 to 0.92, p<0.001); ERR=0.86 (95% CI, 0.81
With the addition of Shockwave, Johnson & Johnson will expand its MedTech cardiovascular portfolio into two of the highest-growth, innovation-oriented segments of cardiovascular intervention – coronaryarterydisease (CAD) and peripheral arterydisease (PAD). The Reducer System has a growing commercial presence.
BackgroundCoronary microvascular dysfunction (CMD), which mimics symptoms of obstructive coronaryarterydisease, has significant prognostic implications. Journal of the American Heart Association, Ahead of Print. Patients with chest computed tomography within 1 year of CMD evaluation were included.
Assessment of patients presenting for the first time with suspected coronaryarterydisease (CAD) remains cumbersome with multiple diagnostic options. Invasive coronary angiography as a first-line test tends to be reserved for patients with high probability of CAD (typical angina symptoms with risk.
The favorable efficacy of CHM was primarily presented on five main conditions, coronaryarterydisease, hypertension, heart failure, restenosis, and angina pectoris. CHM, with or without conventional treatment, showed a consistent beneficial effect in various cardiovascular diseases.
Patients usually have a normal life expectancy unless other structural heart diseases are present. Introduction:Dextrocardia is a rare congenital condition where the heart's apex points to the right, with an incidence of about 0.01%. His vital signs were normal, and the physical examination was unremarkable.
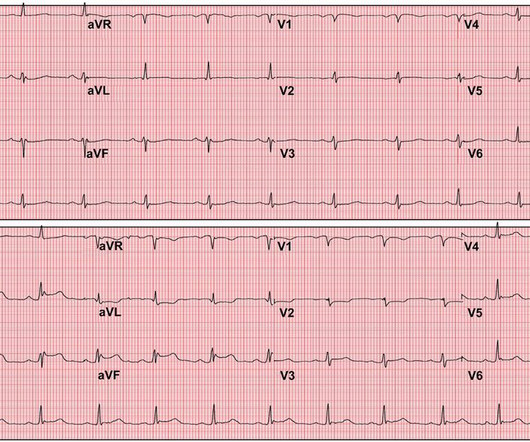
This highlights the need for serial ECGs in acute coronary syndrome as initial ECGs may be near normal even in those with severe disease. Classical electrocardiographic pattern in left main coronaryarterydisease is ST elevation in aVR with extensive ST depression in other leads, most prominent in I, II and V4-V6.
Background:The impact of antianginal therapies on the health status of coronaryarterydisease (CAD) patients who have undergone coronary revascularization has not been extensively researched. Methods:We analyzed data from 1,556 patients enrolled in the GREAT Disease Registry Study (Clinicaltrial No.
Introduction:Inflammation plays an important role in the pathogenesis of coronaryarterydisease and Acute Coronary Syndrome (ACS). Types of ACS include stable angina 5.3% (n=8), unstable angina 24% (n=36), NSTEMI 28.7% (n=43), and STEMI 24% (n=36). The mean age of patients was 57.68 (SD= 11.19) years.
Patient Mr. Paras Ram was having unstable angina (chest pain at rest) at his native place. Coronary angiography showed tight left main coronaryarterydisease with severe triple vessel disease. All his coronaryarteries were heavily calcified.
The primary endpoint consisted of a composite of all-cause mortality, MI, stroke, coronary revascularization, or hospitalization for unstable angina. The results advocate for considering PCI as a treatment option for such plaques, potentially expanding the indications for PCI in coronaryarterydisease management.
I quickly reviewed the patient’s records and saw that she was a 53 year old woman with a history of BMI 40, but no other identifiable risk factors for coronaryarterydisease. The absence of risk factors for coronaryarterydisease does not mean a patient is not at risk for OMI.
For example, if a coronaryartery becomes blocked due to plaque buildup (a condition known as coronaryarterydisease), the heart muscle may not receive enough oxygen, leading to chest pain (angina) or, in more severe cases, a heart attack. Any interruption in this process can result in serious consequences.
Diamond and Forrester accomplished this by first establishing the prevalence of coronaryarterydisease based on how clinically likely patients with chest pain symptoms were found to have coronarydisease based on a coronary angiogram. Thanks for reading Dr. Anish Koka's Newsletter!
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






































Let's personalize your content