This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion.
Clinical introduction Vignette A man in his 40s presented to our emergency department with sudden onset of severe central chestpain radiating to his left arm. There was no antecedent angina. Intravascular ultrasound was also performed ( figure 1B ). He was sweaty, clammy and had accompanying breathlessness.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
He was given aspirin and sublingual nitro and the pain resolved. Bedside cardiac ultrasound with no obvious wall motion abnormalities. Another ECG was recorded after the nitroglycerine and now without pain: All findings are resolved. He had a previous ECG on file: Proving the findings are new The cath lab was activated.
Thus, the patient does not (yet) get a formal diagnosis of MI and must be called unstable angina unless further troponins return above the 99th percentile. The patient said his chestpain was 4/10, down from 8/10 on presentation. On the basis of unresolved angina, cardiology decided to perform rescue PCI. of the time.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
ET Murphy Ballroom 4 Health 360x Registry: Scalable Workforce for Equitable Access to Point of Care Decentralized Clinical Trials Prevalence of Cardiovascular Disease and Risk Factors Among National Football League Alumni and Their Family Members: Results from the Huddle Study Hózhó (Heart Failure Optimization at Home to Improve Outcomes): A Pragmatic (..)
She asked me why I felt she had had a heart attack and I explained to her that she had had chestpains and the blood test indicating damage to the heart was elevated and that was all we needed to say that she had had a heart attack. On the basis of these findings we told her that she had suffered a heart attack.
This case was provided by Spencer Schwartz, an outstanding paramedic at Hennepin EMS who is on Hennepin EMS's specialized "P3" team, a team that receives extra training in advanced procedures such as RSI, thoracostomy, vasopressors, and prehospital ultrasound. Takotsubo is a sudden event, not one with crescendo angina.
3 hours prior to calling 911 he developed typical chestpain. 1.196 x STE60 in V3 in mm) + (0.059 x computerized QTc) - (0.326 x RA in V4 in mm) Third, one can do an immediate cardiac ultrasound. Medics gave him nitroglycerine sublingual and his pain resolved. greater than 23.4 is likely anterior STEMI).
About 5% of patients who present to A+E with chestpain which is not deemed to be a heart attack or angina are ultimately diagnosed with pericarditis. Pericarditis Keywords: Pericarditis; myopericarditis; chestpain; yorkcardiology The post Pericarditis appeared first on Dr Sanjay Gupta Cardiologist.
male with a history of HTN and ETOH developed squeezing epigastric abdominal pain with associated vomiting and diaphoresis, followed by a syncopal episode which lasted about 10 seconds. When medics arrived, he denied any chestpain, shortness of breath, or palpitations prior to the syncopal episode.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. These diagnoses were not found in his medical records nor even a baseline ECG.
He had concurrent sharp substernal chestpain that resolved, but palpitations continued. Over past 3 months, he has had similar intermittent episodes of sharp chestpain while running, but none at rest. Pads were placed with ultrasound guidance, so they were in the correct position. However, this is not SVT.
This was diagnosed by IVUS (intravascular ultrasound) as a ruptured plaque. Therefore this is " Transient ST Elevation Unstable Angina." As there was ruptured plaque, this is NOT Prinzmetal's angina. Here are many other cases of Unstable Angina , in spite of Eugene Braunwald's Requiem for Unstable Angina.
A middle aged patient who was 3 weeks s/p STEMI came from cardiac rehab where he developed some chestpain, dyspnea and weakness on the treadmill. In the ED he had some continued chestpain and hypotension. 5 of 6 presented with chestpain and an ECG indicating reperfusion therapy, but were detected by bedside ultrasound.
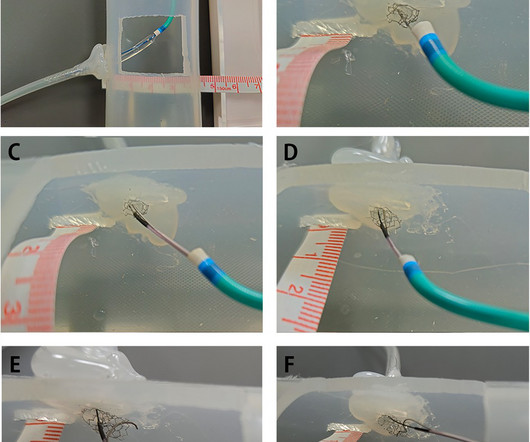
In this article, we introduce a dual-lumen microcatheterfacilitated wiring technique performed on two patients to overcome this difficulty.Case summaryThe first case was a 75-year-old man who presented with chestpain. Despite several attempts, the guidewire passed through the side strut of the stent instead of the central stent lumen.
Written by Willy Frick A man in his 60s with a history of hypertension and 40 pack-year history presented to the ER with 1 day of intermittent, burning substernal chestpain radiating into both arms as well as his back and jaw. Even though guidelines say that patients with high-risk features, refractory angina, instability, etc.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
























Let's personalize your content