This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. Is there STEMI? Fortunately the patient was then taken for angiography.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. What do you think the prehospital ECG showed (with pain)?
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. I sent this to the Queen of Hearts So the ECG is both STEMI negative and has no subtle diagnostic signs of occlusion.
Written by Jesse McLaren, with comments from Smith and Grauer A 60 year old presented with three weeks of intermittent non-exertional chestpain without associated symptoms. A prospective validation of the HEART score for chestpain patients at the emergency department. Backus BE, Six AJ, Kelder JC, et al.
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. So you are going to get to see what the ECG would have shown had you recorded one during pain! Am Heart J.
It has been estimated that in the aggregate, they occur at a rate of about 3 per 1000 patients with acute MI, and most of these events occur in patients with STEMI. A mong patients with STEMI, ventricular septal rupture is the most common and free wall rupture is the least common.
This case was recently posted by Tyron Maartens on Facebook EKG club (he agreed to let me post it here), with the following clinical information: "42 year old male with two weeks of intermittent chest discomfort, awoke 4 hours prior to this ECG with a more severe, heavy chestpain (5/10). Both support acute anterior STEMI.
ChestPain in a 61 year old male. Inferior STEMI without inferior ST elevation. ChestPain in a Male in his 20's; Inferior ST elevation: Inferior lead "early repol" diagnosed. The development of an inferior-posterior STEMI, from prehospital to hospital Case 6. Is this STEMI?
This is a 45 yo male who had an inferior STEMI 6 months prior, was found to have severe LAD and left main disease, and was supposed to be set up for CABG a few weeks later, but did not follow up. 3 hours prior to calling 911 he developed typical chestpain. But it could be anterior STEMI. is likely anterior STEMI).
This appears to be a classic Wellens' ECG, Pattern A, with terminal T-wave inversion in V2-V4, preserved R-waves, and it appears to be Wellens' syndrome, as it occurred after resolution of typical anginapain. Wellens' syndrome represents the aftermath of an unrecorded occlusion (STEMI) with spontaneous reperfusion.
A 40-something male presented with dyspnea and left arm numbness, and perhaps some chest tightness, for 1 1/2 hours. This is all but diagnostic of STEMI, probably due to wraparound LAD The cath lab was activated. Therefore this is " Transient ST Elevation Unstable Angina." Why is this important? JACC 2016;67:1531.
Thus, the patient does not (yet) get a formal diagnosis of MI and must be called unstable angina unless further troponins return above the 99th percentile. The patient said his chestpain was 4/10, down from 8/10 on presentation. On the basis of unresolved angina, cardiology decided to perform rescue PCI. of the time.
A middle-aged woman with history of hypertension presented to another hospital approximately 2 hours after onset of chestpain and shortness of breath. This is technically a STEMI, with 1.5 However, I think many practitioners might not see this as a clear STEMI, and would instead call this "borderline."
This male in his 40's had been having intermittent chestpain for one week. He awoke from sleep with crushing central chestpain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. Type B waves are deeper and symmetric. Lessons: 1. de Zwaan C., Janssen J.H.A.,
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chestpain, lasting 5 minutes at a time, with several episodes over the past couple of months. Plan was for admission for chestpain workup. Jernberg T, et al.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chestpain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. See the list below.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chestpain similar to his prior MI, but worse. The pain initially started the day prior to presentation. The ST elevation from today is ~0.2
Here is his ED ECG at triage: Obvious high lateral OMI that does not quite meet STEMI criteria. He was given aspirin and sublingual nitro and the pain resolved. The history is concerning ( This patient was awakened from sleep by chestpain that persisted for several hours — on a background of intermittent CP in recent weeks ).
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
But beware the few false negatives, especially when there are hyperacute T-waves but no ST elevation (see Case 2 below): Formula to differentiate Normal Variant ST Elevation (Early Repolarization) from Anterior STEMI. 2 or 3 do not rule out unstable angina, even in the era of high sensitivity troponin: this study by Thelin et al.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered. As per Drs.
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chestpain and SOB. She had one episode of pain the previous night and two additional episodes early on morning the morning she presented. Deep breaths are painful and symptoms come and go.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
It is equivalent to a transient STEMI. Not much, but studies of STEMI and NonSTEMI show that about 70% of those diagnosed with STEMI have a peak troponin I above 10 ng/mL and that about 70% of those diagnosed with NonSTEMI have a peak troponin I below 10 ng/mL. Again, cath lab was not activated. Int J Cardiol. 2016;207:341–348.
While this ECG is negative for “posterior STEMI”, the resolution of anterior ST depression (accompanied by the troponin elevation) confirms posterior OMI with spontaneous reperfusion. The second opportunity to make the diagnosis and expedite angiography was missed because the ECG never met STEMI criteria and continued to be labeled ‘normal.’
When total LM occlusion does present with STE in aVR, there is ALWAYS ST Elevation elsewhere which makes STEMI obvious; in other words, STE is never limited to only aVR but instead it is part of a massive and usually obvious STEMI. All are, however, clearly massive STEMI. This is her ECG: An obvious STEMI, but which artery?
A middle-aged woman had intermittent angina for 48 hours, then onset of constant, crushing chestpain for 1.5 cm diameter in the apex The presence of thrombus led the clinicians to state that this was a "late presentation STEMI." hours when she called 911. LV Thrombus , 1.5 0 0 1 95 544 MMRF 4 1 638 14.0
But immediate resolution of chestpain once VT was converted — and — the normal CT coronary angiogram — essentially ruled out acute coronary disease as the cause. Subsequent testing supported the presumption of apical cardiomyopathy as the cause of this patient's sustained VT.
male with a history of HTN and ETOH developed squeezing epigastric abdominal pain with associated vomiting and diaphoresis, followed by a syncopal episode which lasted about 10 seconds. When medics arrived, he denied any chestpain, shortness of breath, or palpitations prior to the syncopal episode.
A middle aged patient who was 3 weeks s/p STEMI came from cardiac rehab where he developed some chestpain, dyspnea and weakness on the treadmill. In the ED he had some continued chestpain and hypotension. There is no acute STEMI. This is diagnostic of recent, reperfused STEMI. Plummer D et al.
Scenario 1 : The patient presents with 24 hours of substernal chestpain. 50% of LAD STEMI have Q-waves by one hour. Smith : In limb leads, the ST vector is towards lead II (STE lead II STE lead III, which is more likely with pericarditis than with STEMI). He presented to the emergency department for evaluation.
Written by Willy Frick A man in his 60s with a history of hypertension and 40 pack-year history presented to the ER with 1 day of intermittent, burning substernal chestpain radiating into both arms as well as his back and jaw. In the world of STEMI, we are incapable of recognizing the first ECG as a false negative.
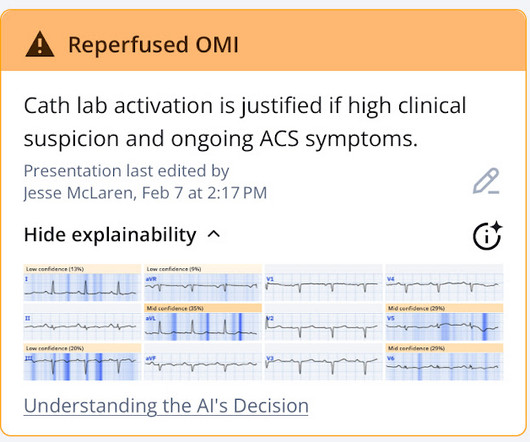
Dizziness is so unlikely to be OMI without an obvious ECG, that I am going to pretend that this patient presented with chestpain. The PMCardio Queen of Hearts app asks you, before giving an interpretation of OMI ("STEMI-Equivalent"), whether the patient's clinical presentation is high risk for OMI. Was it unstable angina?
Written by Jesse McLaren An 80 year old with a history of CHF, ESRD on dialysis, and multiple prior cardiac stents presented to the emergency department with 3 days of intermittent chestpain and shortness of breath that resolved after nitro, which felt like prior episodes of angina. Discharge diagnosis was Non-STEMI.
The fear comes built in with the diagnosis often amplified by young felllows on call (& often times by senior consultants as well) It may appear real, from a clinical angle, but trust, when we deal with the whole gamut of so-called ACS (other than STEMI), there is indeed a benign face in many of them.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content