This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Coronary artery spasm (CAS), or Prinzmetal angina, is a recognised cause of myocardial ischaemia in non-obstructed coronary arteries which typically presents with anginal chestpain. The patient presented with recurrent palpitations and pre-syncope, with no chestpain.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion.
Artery Damage : Hypertension damages the inner lining of your arteries, making them less elastic and more prone to plaque buildup. Coronary Artery Disease (CAD) : High blood pressure accelerates the development of CAD by promoting the buildup of plaques in the coronary arteries.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardial infarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque. The pathologist may see a plaque that constitutes, for example, 50% of the cross-sectional area.
Clinical introduction Vignette A man in his 40s presented to our emergency department with sudden onset of severe central chestpain radiating to his left arm. There was no antecedent angina. The left system showed no disease in the left main stem, but mild plaque disease in the dominant left circumflex artery.
He also complained of intermittent mild chestpain radiating into into both shoulders and his back, as well as occasional unexplained sweating. In addition, his cardiologist suspected vasospastic angina and therefore started amlodipine. He had no further chestpain. The name is self-explanatory.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
Thus, the patient does not (yet) get a formal diagnosis of MI and must be called unstable angina unless further troponins return above the 99th percentile. The patient said his chestpain was 4/10, down from 8/10 on presentation. On the basis of unresolved angina, cardiology decided to perform rescue PCI. Heitner et al.
Case A 42-year-old lady presented to the ED with complaints of intermittent episodes of chestpain associated with shortness of breath for the last 2 days. This was her ECG (it is unclear if this was with or without pain): Computerized ECG Read: “Normal sinus rhythm. Unstable Angina still exists. Thanks, Sam! Normal ECG.”
Whether stenting a narrowed coronary artery improves symptoms such as chestpain (angina) or shortness of breath is a very different question. Share Angina The classic definition of angina involves the sensation of tightness in the centre of the chest that is brought on with exertion and is relieved with rest.
Sustained inflammation can damage your blood vessels, leading to atherosclerosis (plaque buildup) and increasing your risk of heart attack and stroke. This can lead to chestpain (angina) and increase your risk of heart attack or stroke, especially if you already have underlying heart disease.
For example, if a coronary artery becomes blocked due to plaque buildup (a condition known as coronary artery disease), the heart muscle may not receive enough oxygen, leading to chestpain (angina) or, in more severe cases, a heart attack. Any interruption in this process can result in serious consequences.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered. As per Drs.
But the symptoms returned with similar pattern – provoked by exertion, and alleviated with rest; except that on each occasion the chestpain was a little more intense, and the needed recovery period was longer in duration. 3-vessel disease with a culprit lesion [Typical angina, multiple risk factors] b. Severe Hypoxia b.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
She asked me why I felt she had had a heart attack and I explained to her that she had had chestpains and the blood test indicating damage to the heart was elevated and that was all we needed to say that she had had a heart attack. On the basis of these findings we told her that she had suffered a heart attack.
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chestpain and SOB. She had one episode of pain the previous night and two additional episodes early on morning the morning she presented. Deep breaths are painful and symptoms come and go.
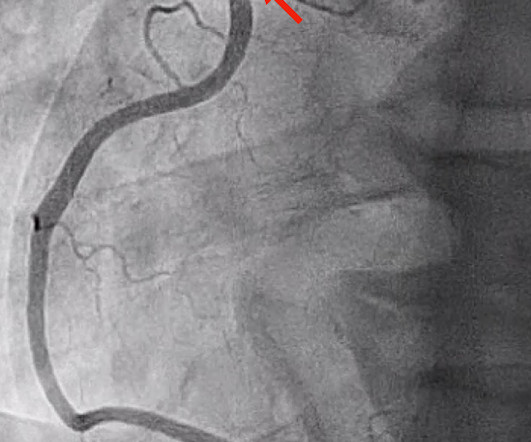
This was diagnosed by IVUS (intravascular ultrasound) as a ruptured plaque. Therefore this is " Transient ST Elevation Unstable Angina." As there was ruptured plaque, this is NOT Prinzmetal's angina. It is just as dangerous, as there is a ruptured plaque with thrombus (which lysed) in the proximal LAD.
ET Murphy Ballroom 4 Health 360x Registry: Scalable Workforce for Equitable Access to Point of Care Decentralized Clinical Trials Prevalence of Cardiovascular Disease and Risk Factors Among National Football League Alumni and Their Family Members: Results from the Huddle Study Hózhó (Heart Failure Optimization at Home to Improve Outcomes): A Pragmatic (..)
Prog- nostic impact of spontaneous coronary artery dissection in young female patients with acute myocardial infarction: a report from the Angina Pecto- ris-Myocardial Infarction Multicenter Investigators in Japan. SCAD occurs in patients with few or non-traditional cardiovascular risk factors. Int J Cardiol. 2016;207:341–348. 2016.01.188.
Written by Willy Frick A woman in her 60s with very severe hyperlipidemia (LDL >200 mg/dL) presented with acute onset chestpain. She described the pain as moderate in severity, and said it had come and gone several times over the next few hours before ultimately resolving. Her symptoms began while getting off the bus.
Written by Willy Frick A man in his 60s with a history of hypertension and 40 pack-year history presented to the ER with 1 day of intermittent, burning substernal chestpain radiating into both arms as well as his back and jaw. Even though guidelines say that patients with high-risk features, refractory angina, instability, etc.
One big chunk of ACS-UA is secondary UA where there is increased demand as in stable angina with tachycardia*. In these patients there is no plaque triggered ACS. I don’t understand how the curve of non-cardiac chestpain trespasses in the middle of a Troponin race (False positives?
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.





























Let's personalize your content