This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Written by Willy Frick A man in his early 40s with BMI 36, hypertension, and a 30 pack-year smoking history presented with three days of chestpain. He described it as a mild intensity, nagging pain on the right side of his chest with nausea and dyspnea. By 6 hours , most of the salvageable myocardium has infarcted.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. These diagnoses were not found in his medical records nor even a baseline ECG.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion. Am Heart J.
This is a value typical for a large subacute MI, n ormal value 48 hours after myocardialinfarction is associated with Post-Infarction Regional Pericarditis ( PIRP ). Mechanical complications secondary to myocardialinfarction are infrequent due to most patients receiving revascularization quite rapidly.
Written by Jesse McLaren, with comments from Smith and Grauer A 60 year old presented with three weeks of intermittent non-exertional chestpain without associated symptoms. A prospective validation of the HEART score for chestpain patients at the emergency department. Backus BE, Six AJ, Kelder JC, et al.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. Electrocardiographic diagnosis of reperfusion during thrombolytic therapy in acute myocardialinfarction.
He also complained of intermittent mild chestpain radiating into into both shoulders and his back, as well as occasional unexplained sweating. Answer: This is MINOCA -- MyocardialInfarction with Non-Obstructive Coronary Arteries. He had no further chestpain. The name is self-explanatory.
This confirms that the pain was ischemia and is now resovled. Thus, it has recently become generally accepted that most plaque ruptures resulting in myocardialinfarction occur in plaques that narrow the lumen diameter by 40% of the arterial cross section may be involved by plaque. The i nitial hs troponin I returned 75%.
The impact of this narrowing can ultimately result in angina (chestpain), which has been shown to double the risk of major cardiovascular events,1 as well as myocardialinfarction ( heart attack ) or even death. Use Heart to Act on Angina. Available at: [link]. Accessed May 2024.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. 1] European guidelines add "regardless of biomarkers". But only 6.4% Clin Cardiol 2022 4. Herman, Meyers, Smith et al.
A middle-aged man complained of 15 minutes of classic angina that resolved upon arrival to the ED. So this is indeed diagnostic of myocardialinfarction. Not immediately, at least, because this is NOT diagnostic of ACUTE (occlusion) myocardialinfarction (Acute OMI). Here is his initial ECG: What do you think?
This male in his 40's had been having intermittent chestpain for one week. He awoke from sleep with crushing central chestpain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. Wellens' syndrome represents a state of reperfusion of the infarct related artery 2.
Manifestations of CVDs, such as chestpain, abnormal serum markers, unstable angina, myocardialinfarction (MI), myocarditis, and new-onset hypertension, were documented. The most common symptom was left hemithorax and interscapular pain (317 patients, 46%).
ET Main Tent (Hall B1) - A Double-blind, Randomized Placebo Procedure-controlled Trial of an Interatrial Shunt in Patients with HFrEF and HFpEF: Principal Results From the RELIEVE-HF Trial - Empagliflozin After Acute MyocardialInfarction: Results of the EMPACT-MI Trial - CSL112 (Apolipoprotein A-I) Infusions and Cardiovascular Outcomes in Patients (..)
Background On the one hand, the primary coronary slow flow phenomenon (CSFP) can cause recurrence of chestpain, prompting medical examinations and further healthcare costs, while on the other hand, it can lead to myocardialinfarction, ventricular arrhythmia and sudden cardiac death.
A man in his 70s with past medical history of hypertension, dyslipidemia, CAD s/p left circumflex stent 2 years prior presented to the ED with worsening intermittent exertional chestpain relieved by rest. This episode of chestpain began 3 hours ago and was persistent even at rest. Troponin was ordered. Eur J Emerg Med.
This means that at every age, the probability a man complaining of chestpain has significant underlying coronary disease as a cause of this chestpain is much higher than a woman complaining of chestpain. The results of this dataset by age and gender follow.
So there is probability of myocardial injury here (and because it is in the correct clinical setting, then myocardialinfarction.) Thus, the patient does not (yet) get a formal diagnosis of MI and must be called unstable angina unless further troponins return above the 99th percentile. Repeat ECG at that time is shown.
This was a male in his 50's with a history of hypertension and possible diabetes mellitus who presented to the emergency department with a history of squeezing chestpain, lasting 5 minutes at a time, with several episodes over the past couple of months. Plan was for admission for chestpain workup. Jernberg T, et al.
Without oxygen, the cells would quickly die, leading to a heart attack (myocardialinfarction). For example, if a coronary artery becomes blocked due to plaque buildup (a condition known as coronary artery disease), the heart muscle may not receive enough oxygen, leading to chestpain (angina) or, in more severe cases, a heart attack.
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chestpain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. BP was 160/100.
A middle-aged woman had an acute onset of chestpain and dyspnea. The pain had almost resolved by the time an ECG was obtained in the ED: Here is the computer diagnosis What do you think? ng/ml , a three-fold increase from troponin #2, also confirming acute myocardialinfarction. It was not normal!
The confirmation cohort, which was obtained from the National Institute of Health, consisted of 3315 patients with normal Bruce protocol treadmill stress test results in the Prospective Multicenter Imaging Study for Evaluation of ChestPain (PROMISE) Trial. RHR and peak exercise heart rates (PHR) were tabulated. x age in years).Results:The
A middle-aged woman with history of hypertension presented to another hospital approximately 2 hours after onset of chestpain and shortness of breath. Early Continuous ST Segment Monitoring in Unstable Angina: Prognostic Value Additional to the Clinical Characteristics and the Admission Electrocardiogram. mm STE in V1 and 1.5-2.0
A middle-aged woman had intermittent angina for 48 hours, then onset of constant, crushing chestpain for 1.5 Appearance of abnormal Q waves early in the course of acute myocardialinfarction: implications for efficacy of thrombolytic therapy. hours when she called 911. These do NOT indicate late, subacute MI.
Therefore, this does not meet the definition of myocardialinfarction ( 4th Universal Definition of MI ), which requires at least one troponin above the 99% reference range. This was clearly severe subepicardial ischemia causing ST Elevation, but it was not of a long enough duration to result in measurable infarct.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
A 34 yo woman with a history of HTN, h/o SVT s/p ablation 2006, and 5 months post-partum presented with intermittent central chestpain and SOB. She had one episode of pain the previous night and two additional episodes early on morning the morning she presented. Deep breaths are painful and symptoms come and go.
The term MINOCA stands for Myocardialinfarction with non-obstructive coronary arteries. A 50-year-old lady was admitted to my hospital with crushing chest tightness. Cardiac Causes Myocarditis – an infection of the heart may cause damage to the heart muscle and cause chestpain.
They were recorded 12 minutes apart: "Hey Steve, 30-something with one week of chestpain, mostly right-sided, better with sitting up.": I do not think this is acute occlusion myocardialinfarction (OMI). This history of a week of constant chestpain is also much more suggestive of myocarditis.
At the bottom of the post, I have re-printed the section on aVR in my article on the ECG in ACS from the Canadian Journal of Cardiology: New Insights Into the Use of the 12-Lead Electrocardiogram for Diagnosing Acute MyocardialInfarction in the Emergency Department Case 1. Widimsky P et al. This was a 100% acute LM occlusion.
This is diagnostic of myocardialinfarction. In middle age women, it accounts for 22-35% of all ACS presentations 1,3 , and the reported incidence of ST-elevation myocardialinfarction in this subset of patients is variable, but estimated to be between 24-50% 4. She felt more comfortable being admitted. Int J Cardiol.
In the STEMI/NSTEMI dichotomy, NSTEMI is supposed to mean non-occlusive myocardialinfarction, but this patient had transient Occlusion MI that was at risk for re-occlusion (like ‘transient STEMI’). Impact of total occluson of culprit artery in acute non-ST elevation myocardialinfarction: a systemic review and meta-analysis.
A middle aged patient who was 3 weeks s/p STEMI came from cardiac rehab where he developed some chestpain, dyspnea and weakness on the treadmill. In the ED he had some continued chestpain and hypotension. Here was his ECG: There are inferior and lateral Q-waves with T-wave inversion in the corresponding leads.
Background In myocardialinfarction with nonobstructive coronary arteries (MINOCA), there are limited patient-level data on outcomes by sex and race. Methods Patients admitted to a single center with acute myocardialinfarction (MI) between 1 January 2012 and 31 December 2018, were identified by chart and angiographic review.
Major findings from the INTERHEART study reveal that stress is more common among cases of acute myocardialinfarction (AMI) compared to controls. As a result, psychological stress is highly associated with CVD and cardiometabolic disease in women. Combining behavioral and pharmacological treatment is most effective.
Risk Factors for ED: Heart disease, specifically coronary artery disease (CAD) and acute myocardialinfarction (AMI), is closely linked to male erectile dysfunction. The aim is to restore proper blood flow to the heart, alleviating symptoms like chestpain (angina) and reducing the risk of heart attacks.
Scenario 1 : The patient presents with 24 hours of substernal chestpain. It could also, given a different clinical context be compatible with a subacute myocardialinfarction complicated by post infarct regional pericarditis. Most common cause) 2 ) Post infarct regional pericarditis. What do you think?
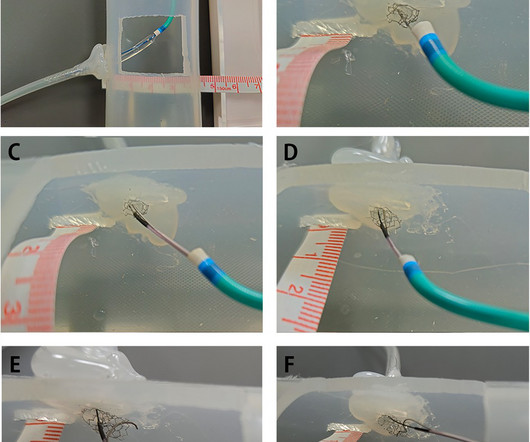
In this article, we introduce a dual-lumen microcatheterfacilitated wiring technique performed on two patients to overcome this difficulty.Case summaryThe first case was a 75-year-old man who presented with chestpain. The second case was a 78-year-old woman diagnosed with non-ST segment elevation myocardialinfarction.
Written by Willy Frick A man in his 60s with a history of hypertension and 40 pack-year history presented to the ER with 1 day of intermittent, burning substernal chestpain radiating into both arms as well as his back and jaw. Even though guidelines say that patients with high-risk features, refractory angina, instability, etc.
A 50-something man presented with worsening severe exertional chestpain which was just resolving as he had an ECG recorded in triage. Are the T-waves in leads I and II hyperacute? Hard to tell. How can we know? By the evolution of the ECG! Watch what happends as the heart recovers from its episode of ischemia.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.










































Let's personalize your content