This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
It is not always possible to be certain about the origin of chestpain just by its characteristics as the variation between individuals is quite a bit. A medical opinion should be sought in case of any significant chestpain so that important ailment is not missed. A pain lasting more than 30 minutes is usual.
Clinical introduction A man in his 40s with a history of hyperlipidaemia presented with intermittent, dull left-sided chestpain for 2 weeks that was not consistently exertional. Physical examination, an ECG, basic laboratories and a chest X-ray were unremarkable. He did not smoke or use alcohol or illicit drugs.
BackgroundVasospastic angina usually presents with intermittent episodes of chestpain. It can rarely be associated with the perception of phantom odors.Case summaryA 69-year-old woman presented for evaluation of intermittent shortness of breath and chestpain.
We aimed to identify non-ischemic phenotypes in low-risk NSTE-ACS patients by analyzing a wide range of parameters available during exercise SE.MethodsInpatients [n=103, median age 56 (4665)years, 65 (63%) men] with suspected NSTE-ACS without high-risk criteria underwent exercise SE using a semi-supine cycle ergometer.
This condition reduces blood flow to the heart, increasing the risk of angina (chestpain) and heart attacks. Exercise Regularly : Aim for at least 150 minutes of moderate-intensity aerobic activity per week, such as walking, cycling, or swimming.
Results from the open label roll-in cohort of patients having chronic myocardial ischemia with refractory angina showed an average increase in exercise tolerance of 107 seconds and an average of 82% reduction in angina episodes at the primary six-month follow-up endpoint compared to before receiving the study treatment.
Written by Jesse McLaren, with comments from Smith and Grauer A 60 year old presented with three weeks of intermittent non-exertional chestpain without associated symptoms. A prospective validation of the HEART score for chestpain patients at the emergency department. Backus BE, Six AJ, Kelder JC, et al.
1 2 The exercise ECG, once the stalwart of chestpain evaluation, has lost favour over the last two decades in most heart centres due to its relatively poor discriminatory ability and reliance on patients to walk on a treadmill.
He had concurrent sharp substernal chestpain that resolved, but palpitations continued. Over past 3 months, he has had similar intermittent episodes of sharp chestpain while running, but none at rest. Episodes of angina over past couple of months had been progressive. Repeat cardioversion was then s uccessful.
Whether stenting a narrowed coronary artery improves symptoms such as chestpain (angina) or shortness of breath is a very different question. Share Angina The classic definition of angina involves the sensation of tightness in the centre of the chest that is brought on with exertion and is relieved with rest.
He described the symptom as chest burning with occasional radiation into his throat and jaw. He first noticed it while exercising. The day of presentation, the pain woke him from sleep, which is why he decided to come in. The patient said his chestpain was 4/10, down from 8/10 on presentation. of the time.
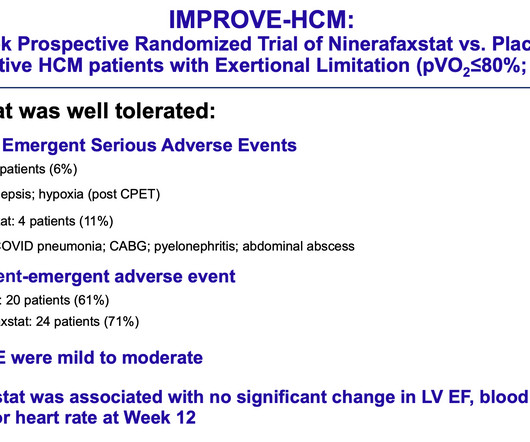
Maron, MD “Our findings provide enthusiasm that a novel drug therapy with ninerafaxstat may provide nonobstructive HCM patients an opportunity to achieve a better quality of life by decreasing symptom burden and improving exercise capacity,” said Martin S. The study was funded by Imbria Pharmaceuticals, developer of ninerafaxstat.
The history is concerning ( This patient was awakened from sleep by chestpain that persisted for several hours — on a background of intermittent CP in recent weeks ). The ECG changes seen between the initial ECG and the repeat ECG after NTG — are undeniable!
This can lead to chestpain (angina) and increase your risk of heart attack or stroke, especially if you already have underlying heart disease. Techniques like regular exercise, deep breathing, meditation, and seeking social support can help you manage stress more effectively and mitigate its cardiovascular impacts.
Background:Cardiac output reserve and exercise capacity are strong predictors of life expectancy. Chronotropic incompetence (CI) is the inability to reach an age appropriate maximum heart rate with exercise. CI reduces cardiac output reserve and exercise capacity, both of which increase all-cause mortality risk. x age in years).Results:The
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chestpain similar to his prior MI, but worse. The pain initially started the day prior to presentation. LAD occlusion. Great case.
For example, if a coronary artery becomes blocked due to plaque buildup (a condition known as coronary artery disease), the heart muscle may not receive enough oxygen, leading to chestpain (angina) or, in more severe cases, a heart attack. CAD is one of the leading causes of heart attacks.
ET Murphy Ballroom 4 Health 360x Registry: Scalable Workforce for Equitable Access to Point of Care Decentralized Clinical Trials Prevalence of Cardiovascular Disease and Risk Factors Among National Football League Alumni and Their Family Members: Results from the Huddle Study Hózhó (Heart Failure Optimization at Home to Improve Outcomes): A Pragmatic (..)
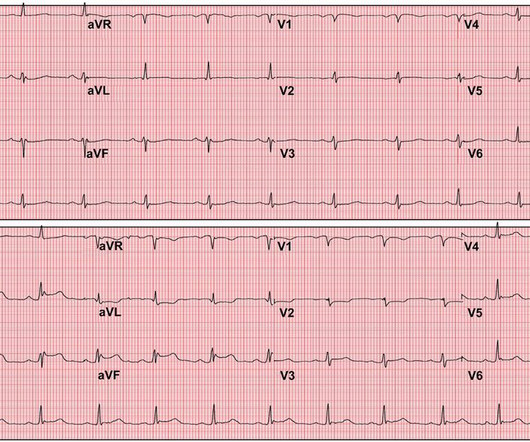
The ECG in Figure-1 was obtained from a previously healthy middle-aged man — who while performing his regular exercise routine, developed "slight" chest discomfort and "palpitations". These symptoms persisted for over an hour, which led the patient to contact EMS.
male with a history of HTN and ETOH developed squeezing epigastric abdominal pain with associated vomiting and diaphoresis, followed by a syncopal episode which lasted about 10 seconds. When medics arrived, he denied any chestpain, shortness of breath, or palpitations prior to the syncopal episode.
Results revealed that women are twice as likely to exhibit myocardial ischemia in response to mental stress compared to traditional stressors like exercise or pharmacologic stress. Moreover, women under 50 years old are four times more likely to experience MSIMI. Combining behavioral and pharmacological treatment is most effective.
Lifestyle Habits: Obesity, smoking, excessive alcohol consumption, and lack of exercise can all negatively impact sexual function. The aim is to restore proper blood flow to the heart, alleviating symptoms like chestpain (angina) and reducing the risk of heart attacks.
BackgroundPainful left bundle branch block (LBBB) syndrome is an uncommon disease that is defined as intermittent episodes of angina associated with simultaneous LBBB changes on an electrocardiogram (ECG) with the absence of flow-limiting coronary artery disease or ischemia on functional testing.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.



























Let's personalize your content