This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Coronary artery spasm (CAS), or Prinzmetal angina, is a recognised cause of myocardial ischaemia in non-obstructed coronary arteries which typically presents with anginal chestpain. The patient presented with recurrent palpitations and pre-syncope, with no chestpain.
Written by Willy Frick A man in his early 40s with BMI 36, hypertension, and a 30 pack-year smoking history presented with three days of chestpain. He described it as a mild intensity, nagging pain on the right side of his chest with nausea and dyspnea. This is WHY refractory angina should prompt immediate angiography.
Written by Colin Jenkins and Nhu-Nguyen Le with edits by Willy Frick and by Smith A 46-year-old male presented to the emergency department with 2 days of heavy substernal chestpain and nausea. The patient continued having chestpain. These diagnoses were not found in his medical records nor even a baseline ECG.
A 50-something male with hypertension and 20- to 40-year smoking history presented with 1 week of stuttering chestpain that is worse with exertion, which takes many minutes to resolve after resting and never occurs at rest. At times the pain does go to his left neck. It is a ssociated with mild dyspnea on exertion.
(MedPage Today) -- PARIS -- Whether a person had chestpains resolved by angioplasty hinged on the nature, not the severity, of their presenting symptoms, an ORBITA-2 analysis showed. Investigators found two groups more likely to benefit from.
It is not always possible to be certain about the origin of chestpain just by its characteristics as the variation between individuals is quite a bit. A medical opinion should be sought in case of any significant chestpain so that important ailment is not missed. A pain lasting more than 30 minutes is usual.
Clinical introduction A man in his 40s with a history of hyperlipidaemia presented with intermittent, dull left-sided chestpain for 2 weeks that was not consistently exertional. Physical examination, an ECG, basic laboratories and a chest X-ray were unremarkable. He did not smoke or use alcohol or illicit drugs.
BackgroundVasospastic angina usually presents with intermittent episodes of chestpain. It can rarely be associated with the perception of phantom odors.Case summaryA 69-year-old woman presented for evaluation of intermittent shortness of breath and chestpain.
A coronary sinus reducer (CSR) may lead to a significant reduction in the number of angina episodes in patients with chronic chestpain, but it was not superior to a placebo device for improving myocardial blood flow, according to the results of the ORBITA-COSMIC study, presented during a Late-Breaking Clinical Trial session at ACC.24
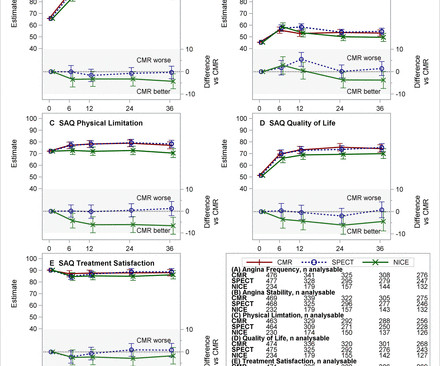
Aims Guidelines for suspected cardiac chestpain have used historical risk stratification tools, advocating invasive coronary angiography (ICA) first-line in those at highest risk. 12) Questionnaire and EuroQol-5 Dimension Questionnaire were recorded.
Results from the open label roll-in cohort of patients having chronic myocardial ischemia with refractory angina showed an average increase in exercise tolerance of 107 seconds and an average of 82% reduction in angina episodes at the primary six-month follow-up endpoint compared to before receiving the study treatment.
This condition reduces blood flow to the heart, increasing the risk of angina (chestpain) and heart attacks. Coronary Artery Disease (CAD) : High blood pressure accelerates the development of CAD by promoting the buildup of plaques in the coronary arteries.
Written by Jesse McLaren, with comments from Smith and Grauer A 60 year old presented with three weeks of intermittent non-exertional chestpain without associated symptoms. A prospective validation of the HEART score for chestpain patients at the emergency department. Backus BE, Six AJ, Kelder JC, et al.
Clinical introduction Vignette A man in his 40s presented to our emergency department with sudden onset of severe central chestpain radiating to his left arm. There was no antecedent angina. He was sweaty, clammy and had accompanying breathlessness. There was no medical history and he was not on any medical treatment.
He had suffered a couple bouts of typical chestpain in the last 24 hours. This ECG (ECG #3) was recorded immediately after the last episode of pain spontaneously resolved. The pain had lasted about one hour. Case A 40-something male presented to triage. There are classic Wellens' waves in V2-V5. Am Heart J.
A 63 year old man with a history of hypertension, hyperlipidemia, prediabetes, and a family history of CAD developed chestpain, shortness of breath, and diaphoresis after consuming a large meal at noon. He called EMS, who arrived on scene about two hours after the onset of pain to find him hypertensive at 220 systolic.
This is NOT Wellens because the T-wave inversion is DURING the pain (not after -- Wellens' is a syndrome of TWI after an episode of angina is resolved). While I still had questions about this case given the limited information provided ( ie, Was chestpain in this younger adult diabetic from acute PE?
He also complained of intermittent mild chestpain radiating into into both shoulders and his back, as well as occasional unexplained sweating. In addition, his cardiologist suspected vasospastic angina and therefore started amlodipine. He had no further chestpain. Clear inferior and posterior reperfusion.
Because previous ischemia induces myocardial preconditioning, decreasing the likelihood of transmural myocardial necrosis and myocardial rupture, patients with evidence of diabetes mellitus, chronic angina or previous MI are less likely to experience a rupture. Not all patients with acute ( or recent ) MI have chestpain with their event.
Patients experiencing LVOTO may manifest symptoms such as angina, syncope, etc. Our report describes two cases of SVS treated with endocardial ablation to improve LVOTO.Case reportCase 1: A 74-year-old female patient with angina and syncope was admitted to the hospital and diagnosed with SVS by transthoracic echocardiogram.
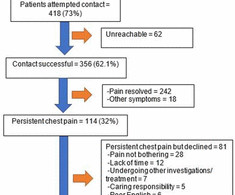
Objective The study evaluated the feasibility of mindfulness-based cognitive therapy (MBCT) in patients with non-cardiac chestpain by assessing their willingness to participate and adhere to the programme, and for these data to help further refine the content of MBCT for chestpain. ±7.3).
A middle-aged man complained of 15 minutes of classic angina that resolved upon arrival to the ED. The patient's chestpain had resolved by the time of the ECG 2. But it does prove that the patient has coronary disease and makes the probability that his chestpain is due to ACS very very high. The T-waves are flat.
The impact of this narrowing can ultimately result in angina (chestpain), which has been shown to double the risk of major cardiovascular events,1 as well as myocardial infarction ( heart attack ) or even death. Use Heart to Act on Angina. Available at: [link]. Accessed May 2024.
Written by Jesse McLaren A 70 year old with prior MIs and stents to LAD and RCA presented to the emergency department with 2 weeks of increasing exertional chestpain radiating to the left arm, associated with nausea. 1] European guidelines add "regardless of biomarkers". But only 6.4%
This appears to be a classic Wellens' ECG, Pattern A, with terminal T-wave inversion in V2-V4, preserved R-waves, and it appears to be Wellens' syndrome, as it occurred after resolution of typical anginapain. The patient remained pain free. Unstable Angina still exists 2. Case continued All troponins were negative.
ChestPain in a 61 year old male. ChestPain in a Male in his 20's; Inferior ST elevation: Inferior lead "early repol" diagnosed. A Case of Clinical Unstable Angina in the ED This case shows how hyperacute is only relative to the baseline T-waves. Details in every case make it even better, so click on the link!!
The patient was suffering with angina (chestpain) since 2002. He was now getting chestpain even at rest and his life was at grave risk. He received these 12 stents on 5 different occasions at 5 different hospitals of the twin cities. The last 3 stents were placed just 6 months back but were not working.
Case A 42-year-old lady presented to the ED with complaints of intermittent episodes of chestpain associated with shortness of breath for the last 2 days. This was her ECG (it is unclear if this was with or without pain): Computerized ECG Read: “Normal sinus rhythm. Unstable Angina still exists. Thanks, Sam! Normal ECG.”
This means that at every age, the probability a man complaining of chestpain has significant underlying coronary disease as a cause of this chestpain is much higher than a woman complaining of chestpain. The results of this dataset by age and gender follow.
Chestpain or discomfort) What do you think? The total duration of chestpain was 30-45 minutes. I said that this is unstable angina until proven otherwise. Thus, Unstable Angina. Here was my response: "Suspicious for inferior posterior OMI. I said "give aspirin, heparin, and troponins will be positive."
Whether stenting a narrowed coronary artery improves symptoms such as chestpain (angina) or shortness of breath is a very different question. Share Angina The classic definition of angina involves the sensation of tightness in the centre of the chest that is brought on with exertion and is relieved with rest.
Manifestations of CVDs, such as chestpain, abnormal serum markers, unstable angina, myocardial infarction (MI), myocarditis, and new-onset hypertension, were documented. The most common symptom was left hemithorax and interscapular pain (317 patients, 46%).
Objectives There are few reports regarding the prognosis in patients with obstructive coronary artery disease (OCAD) and vasospastic angina (VSA). This study investigated the clinical characteristics and clinical outcomes in patients with VSA and OCAD, especially regarding provoked spasm phenotypes and sites.
Hemant, a resident of Delhi NCR, had developed chestpain (angina). However, within 3 months of stenting, he developed increasing chestpain. He underwent coronary angiography at Delhi, which showed severe blocks in left main and other coronary arteries of his heart.
He had concurrent sharp substernal chestpain that resolved, but palpitations continued. Over past 3 months, he has had similar intermittent episodes of sharp chestpain while running, but none at rest. Episodes of angina over past couple of months had been progressive. Repeat cardioversion was then s uccessful.
Thus, the patient does not (yet) get a formal diagnosis of MI and must be called unstable angina unless further troponins return above the 99th percentile. The patient said his chestpain was 4/10, down from 8/10 on presentation. On the basis of unresolved angina, cardiology decided to perform rescue PCI. of the time.
This male in his 40's had been having intermittent chestpain for one week. He awoke from sleep with crushing central chestpain and called ems. EMS recorded a 12-lead, then gave 2 sublingual nitros with complete relief of pain. Type B waves are deeper and symmetric. Lessons: 1. de Zwaan C., Janssen J.H.A.,
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
1 2 The exercise ECG, once the stalwart of chestpain evaluation, has lost favour over the last two decades in most heart centres due to its relatively poor discriminatory ability and reliance on patients to walk on a treadmill.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chestpain similar to his prior MI, but worse. The pain initially started the day prior to presentation. The ST elevation from today is ~0.2
Background On the one hand, the primary coronary slow flow phenomenon (CSFP) can cause recurrence of chestpain, prompting medical examinations and further healthcare costs, while on the other hand, it can lead to myocardial infarction, ventricular arrhythmia and sudden cardiac death.
63 years old Afsar Khan resident of Karwan, Hyderabad had been having coronary artery disease and chestpain on exertion for about a year. However, after discharge from hospital, his heart symptoms increased and in May he developed unstable angina. With increasing chestpain, he underwent coronary angiography in June.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.











































Let's personalize your content