This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
BackgroundSigmoid Ventricular Septum (SVS) is a type of hypertrophic cardiomyopathy characterized by a reduced angle between the basal interventricular septum and the ascending aorta, and SVS can lead to dynamic Left Ventricular Outflow Tract obstruction (LVOTO) during hypercontractile states.
A middle-aged man complained of 15 minutes of classic angina that resolved upon arrival to the ED. The patient's chestpain had resolved by the time of the ECG 2. But it does prove that the patient has coronary disease and makes the probability that his chestpain is due to ACS very very high. The T-waves are flat.
This appears to be a classic Wellens' ECG, Pattern A, with terminal T-wave inversion in V2-V4, preserved R-waves, and it appears to be Wellens' syndrome, as it occurred after resolution of typical anginapain. The patient remained pain free. Unstable Angina still exists 2. Case continued All troponins were negative.
link] A 62 year old man with a history of hypertension, type 2 diabetes mellitus, and carotid artery stenosis called 911 at 9:30 in the morning with complaint of chestpain. He described it as "10/10" intensity, radiating across his chest from right to left. This is written by Willy Frick, an amazing cardiology fellow in St.
She asked me why I felt she had had a heart attack and I explained to her that she had had chestpains and the blood test indicating damage to the heart was elevated and that was all we needed to say that she had had a heart attack. On the basis of these findings we told her that she had suffered a heart attack.
This patient, who is a mid 60s female with a history of hypertension, hyperlipidemia and GERD, called 911 because of chestpain. A mid 60s woman with history of hypertension, hyperlipidemia, and GERD called 911 for chestpain. It is also NOT the clinical scenario of takotsubo (a week of intermittent chestpain).
Subsequent testing supported the presumption of apical cardiomyopathy as the cause of this patient's sustained VT. ie, Severe subendocardial ischemia from sustained VT in a patient severe apical cardiomyopathy resulted in a peak troponin >31,000 ng/L in today's case ). CT coronary angiogram showed no obstructive coronary disease.
Troponins may be negative with very rapid reperfusion, or measured too late, or chronically elevated due to cardiomyopathy or renal failure. While ST coving in V1 is not necessarily abnormal — the presence of ST elevation in association with ST-T wave abnormalities in V2,V3 in a patient with chestpain is clearly cause for concern.
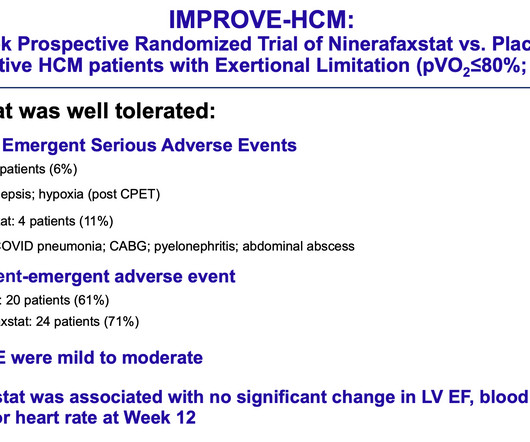
Maron, MD , a cardiologist and director of the Hypertrophic Cardiomyopathy Center at Lahey Hospital and Medical Center in Burlington, Massachusetts, and the study’s lead author. For more information on hypertrophic cardiomyopathy, visit CardioSmart.org/HCM. The safety and tolerability of the drug in this phase 2 trial was excellent.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.
















Let's personalize your content