This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
BackgroundSigmoid Ventricular Septum (SVS) is a type of hypertrophic cardiomyopathy characterized by a reduced angle between the basal interventricular septum and the ascending aorta, and SVS can lead to dynamic Left Ventricular Outflow Tract obstruction (LVOTO) during hypercontractile states.
A middle-aged man complained of 15 minutes of classic angina that resolved upon arrival to the ED. It is proven better than angiography alone in stable angina , and also has been shown to improve decisions on stenting non-culprit lesions in ACS. Here is his initial ECG: What do you think?
Hypertrophic cardiomyopathy is a genetic disorder with a guarded prognosis which occurs in about 1:500 individuals. The most common symptom of hypertrophic cardiomyopathy is dyspnoea which occurs in 90% of cases and is due to elevated left ventricular diastolic pressures as a consequence of the diastolic dysfunction.
The commonest causes of MINOCA include: atherosclerotic causes such as plaque rupture or erosion with spontaneous thrombolysis, and non-atherosclerotic causes such as coronary vasospasm (sometimes called variant angina or Prinzmetal's angina), coronary embolism or thrombosis, possibly microvascular dysfunction.
Given her lack of risk factors for coronary disease, and the fact that she was a 53 year old woman with compatible history and echo findings, stress cardiomyopathy rose to the top of my differential. Of course, stress cardiomyopathy is a diagnosis of exclusion. But it is a diagnosis of exclusion.
This appears to be a classic Wellens' ECG, Pattern A, with terminal T-wave inversion in V2-V4, preserved R-waves, and it appears to be Wellens' syndrome, as it occurred after resolution of typical angina pain. When this happens, troponins are negative, there is no wall motion abnormality, and it is true unstable angina.
However some patients can develop heart failure, angina, and arrhythmia due to significant intracardiac shunt or coronary steal phenomenon. In this case presentation, it is likely that his heart failure was caused by the significant left to right shunt due to the fistula.
Subsequent testing supported the presumption of apical cardiomyopathy as the cause of this patient's sustained VT. ie, Severe subendocardial ischemia from sustained VT in a patient severe apical cardiomyopathy resulted in a peak troponin >31,000 ng/L in today's case ). CT coronary angiogram showed no obstructive coronary disease.
Then I think it is important that patient has an assessment of the function of the heart by means of an ultrasound to look for cardiomyopathies, Takotsubo etc. MINOCA – When a heart attack is not a heart attack Keywords: MINOCA; MI with normal coronary arteries; Coronary vasospasm; Microvascular angina; Syndrome X; Prinzmetal angina.
by making it clear to everyone that this is NOT an EKG that one sees with takotsubo cardiomyopathy. Takotsubo is a sudden event, not one with crescendo angina. The impact of ST-segment elevation on the prognosis of patients with Takotsubo cardiomyopathy. I need to innoculate you against the subsequent opinions below.
Troponins may be negative with very rapid reperfusion, or measured too late, or chronically elevated due to cardiomyopathy or renal failure. Angiograms may be negative due to spasm or thrombus lysis or small vessel disease, or it may be a type 2 MI. Int J Cardiol. 2016;207:341–348. doi: 10.1016/j.ijcard.2016.01.188. 2016.01.188.
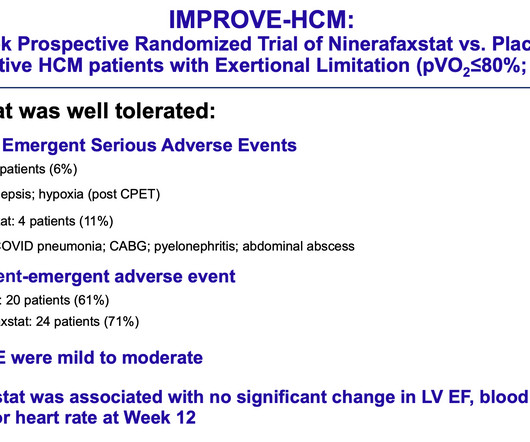
Maron, MD , a cardiologist and director of the Hypertrophic Cardiomyopathy Center at Lahey Hospital and Medical Center in Burlington, Massachusetts, and the study’s lead author. For more information on hypertrophic cardiomyopathy, visit CardioSmart.org/HCM. The safety and tolerability of the drug in this phase 2 trial was excellent.
MACEs included allcause death, recurrent myocardial infarction, stroke, heart failure, atrial fibrillation, and angina pectoris. LA and left ventricular strains varied by pathogenesis, with the lowest strain in patients with cardiomyopathy. This study included 386 patients, with a median time from admission to CMR of 4 days.
Patients receiving semaglutide showed a greater change in Kansas City Cardiomyopathy Questionnaire (KCCQ) clinical summary scores at 52 weeks than placebo. The primary endpoint consisted of a composite of all-cause mortality, MI, stroke, coronary revascularization, or hospitalization for unstable angina. in the medical therapy group.
If our valves are leaky then again, a smaller volume of blood is effectively ejected because some leaks back Cardiomyopathies – if the heart muscle itself is defective in some way then that makes it weaker. This includes conditions like familial hypertrophic cardiomyopathy, familial dilated cardiomyopathy etc.
How common is angina in DCM ? Angina in DCM is an exception despite elevated LVEDP. Is the above logic explain why very few dilated cardiomyopathy patients experience angina? Even in ischemic cardiomyopathy, once it sets in, Intensity of angina is mitigated or completley eliminated.(of
The study presents a case of INOCA attributed to CMVD in a 53-year-old male patient experiencing exertional angina, despite the absence of significant coronary artery stenosis on angiography. While an MYH7 variant was also detected, its clinical relevance was ruled out due to the family's absence of associated cardiomyopathy phenotypes.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content