This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
Coronary artery spasm (CAS), or Prinzmetal angina, is a recognised cause of myocardial ischaemia in non-obstructed coronary arteries which typically presents with anginal chest pain. The arrhythmias persisted despite initial medical management, including calcium channel blockers and intravenous glyceryl trinitrate.
There are three mechanisms of arrhythmia: automatic, re-entry, and triggered. The most common triggered arrhythmia is Torsades de Pointes. It is a benign arrhythmia which requires no specific treatment. Possible mechanisms of ventricular arrhythmias elicited by ischemia followed by reperfusion. What is the rhythm?
with ST elevated myocardial infarction (STEMI), 3.41% with unstable angina, 0.56% with stable angina, and 0.11% were diagnosed with various types of arrhythmias. Approximately 48.5% of the patients were diagnosed with non-ST elevated myocardial infarction (NSTEMI), 36.8% There were initially 65.2%
The disease can cause a variety of symptoms, including heart failure, arrhythmias, peripheral embolism, dysautonomia, angina with normal coronary arteries, and others. The aim of this thematic collection is to gather high-quality articles that contribute to the advancement of knowledge about cardiac amyloidosis.
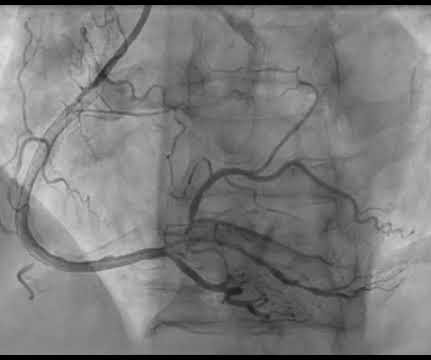
Thus, the patient does not (yet) get a formal diagnosis of MI and must be called unstable angina unless further troponins return above the 99th percentile. On the basis of unresolved angina, cardiology decided to perform rescue PCI. Medically refractory angina should have immediate angiography, but this only happens 6.4%
Sympathectomy or spinal cord stimulation for the treatment of angina pectoris, as well as cardiac sympathetic denervation for the treatment of long QT syndrome associated with malignant ventricular arrhythmias, have been available and performed for more than half a century.
Arrhythmias (Abnormal Heart Rhythms) Stress hormones can disrupt the signals that regulate your heartbeat, leading to arrhythmias – abnormal heart rhythms that cause your heart to beat too fast, too slow, or irregularly.
Background On the one hand, the primary coronary slow flow phenomenon (CSFP) can cause recurrence of chest pain, prompting medical examinations and further healthcare costs, while on the other hand, it can lead to myocardial infarction, ventricular arrhythmia and sudden cardiac death.
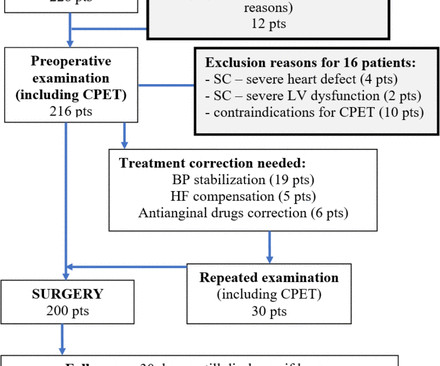
Results 200 patients (mean age 68±14.2 years) met inclusion and exclusion criteria: oesophageal surgery 54 pts, gastric surgery 132 pts and combined oesophageal/gastric surgery 14 pts. to 22.47).
Therefore this is " Transient ST Elevation Unstable Angina." As there was ruptured plaque, this is NOT Prinzmetal's angina. Here are many other cases of Unstable Angina , in spite of Eugene Braunwald's Requiem for Unstable Angina. So Unstable Angina still exists [even with high sensitivity (hs) troponins].
However some patients can develop heart failure, angina, and arrhythmia due to significant intracardiac shunt or coronary steal phenomenon. Patient was planned to gradually start cardiac rehab.Discussion:CCF is a rare anomalous connection between coronary arteries and a cardiac chamber or other major blood vessels of the heart.
Angina is another common symptom due the hypertrophy which causes a coronary supply demand mismatch Symptoms of HCM include syncope/near syncope, which could be precipitated by exertion, hypovolemia, rapid standing, Valsalva manoeuvre, diuretics, vasodilators or arrhythmia. Palpitations can be felt if there are arrhythmias.
Measurement of QT interval is very important, as QT prolongation can predispose to serious, life threatening ventricular arrhythmias. QT prolongation leads to torsades des pointes, which is a very serious arrhythmia. That is usually with angina and ventricular strain patterns. One easy value which I remember is 0.34
A middle aged male with no h/o CAD presented with one week of crescendo exertional angina, and had chest pain at the time of the first ECG: Here is the patient's previous ECG: Here is the patient's presenting ED ECG: There is isolated ST depression in precordial leads, deeper in V2 - V4 than in V5 or V6. There is no ST elevation.
The finding of all negative QRS complexes in leads V3-thru- V6 therefore strongly suggests that the arrhythmia-associated impulse is not traveling over an AP ( Steurer et al — Clin. This should result in at least some positivity of QRS complexes as one moves toward the lateral chest leads. Cardiol 17:306-308, 1994 ).
Findings also confirm previous healthy volunteer trials with IR NIC highlighting no tendency promoting arrhythmia in normal, non-ischemic myocardium. While EU labeling and trials highlight no proarrhythmogenicity lack of recent data remains along with prior reports of potential impact of IR NIC on EKG patterns.
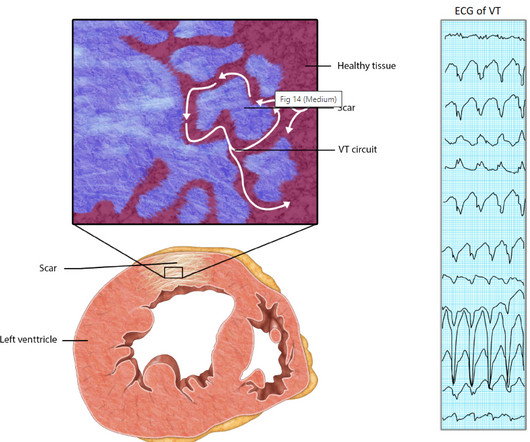
Relationship between Ischemia and arrhythmia While the relationship between Ischemia and VT is really complex, the term “Ischemic VT” itself adds more twists. In chronic VT , shooting down the ischemic focus by ablation its more likely to extinguish the arrhythmia ,rather than revascularization.
On Sunday, the patient complained of dyspnea and angina while ambulating. Initial hsTnI was 14,114 ng/L, repeat 12,651 ng/L, none further checked. Echocardiogram showed inferior wall hypokinesis. The patient was evaluated Saturday with no changes to plan. Repeat ECG is shown.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.






















Let's personalize your content