This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
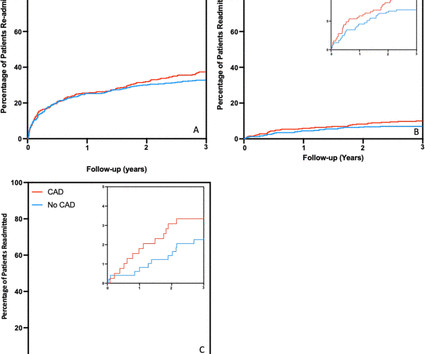
Background Aortic stenosis is a life-limiting condition for which transcatheter aortic valve implantation (TAVI) is an established therapy. Subsidiary outcomes included patient angina and breathlessness scores. CAD at the time of TAVI also did not alter breathlessness or angina scores before/after TAVI (p>0.05).
This potential vascular market for this product family is measured in millions of procedures per year, including cardiac interventions such as structural heart procedures and electrophysiology procedures, peripheral vascular interventions including renal interventions, endovascular aortic repair, and carotid artery interventions.
Given radiation of pain into the patient's back, he underwent CTA which showed no evidence of aortic dissection or any other acute pathology. Recall that medically refractory angina is itself a Class I indication for immediate angiography (see Figure 8). This is WHY refractory angina should prompt immediate angiography.
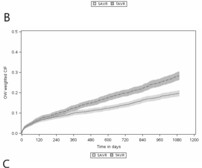
Background and aims Randomised controlled trials comparing transcatheter aortic valve replacement (TAVR) and surgical aortic valve replacement (SAVR) were performed in highly selected populations and data regarding long-term secondary complications beyond mortality are scarce. All-cause mortality at 1 year (HR 1.21; 95% CI 1.02
24: Joint American College of Cardiology/Journal of the American College of Cardiology Late-Breaking Clinical Trials (Session 402) Saturday, April 6 9:30 – 10:30 a.m.
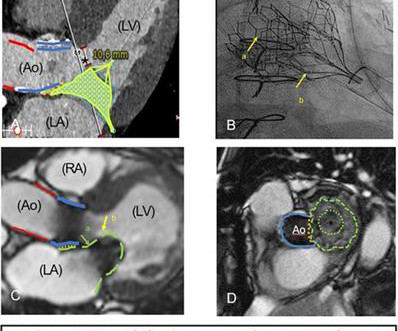
Prior transapical transcatheter aortic valve replacement (TA-TAVR) may complicate the procedure and is therefore considered a relative contraindication. Pre-operative CT suggested good alignment of the aortic and mitral valved stent which was confirmed postoperatively.
The patient was referred for an exercise nuclear study and did 11 min on the Bruce protocol without angina or ischaemic ECG changes. Aortic dissection Sinus of Valsalva aneurysm Anomalous coronary artery Unroofed. Myocardial scintigraphic perfusion images at stress and rest were normal. Question What is the most likely diagnosis?
The Queen of Hearts disagrees, diagnosing OMI with high confidence: Case Continued: The EKG was not immediately recognized by the emergency provider, who ordered a CT scan to rule out aortic dissection at 1419. If it is angina, lowering the BP with IV Nitroglycerine may completely alleviate the pain and the (unseen) ECG ischemia.
Given the consistency of the clinical profile with typical angina, associated risk factors, and abnormal ECG findings, a cardiology consult was promptly requested. Aortic Stenosis f. Aortic Stenosis [No Hx syncope, and no systolic murmur] f. 3-vessel disease with a culprit lesion [Typical angina, multiple risk factors] b.
The typical pain of cardiac origin is a central chest pain which occurs on walking or other forms of exercise, known as effort angina. Effort angina is commonly due to significant obstruction to a blood vessel (coronary artery) supplying a part of the heart muscle. Pain is likely to be more if you are walking after a heavy meal.
Left ventricular afterload reduction is essential to decrease the trans-se ptal pressure gradient and thus decrease shunt volume, making a larger proportion of the blood flow from the left ventricle through the aortic valve. Surgical repair of the VSR was eventually done.
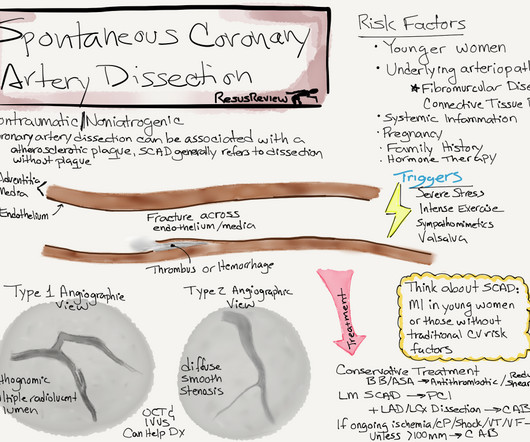
may be misdiagnosed as post infarct angina. This has important clinical significance , as many successfully lysed STEMI patient might have minimal segments of dissection/deep plaque fissures. , Spontaneous coronary dissection vs Iatrogenic dissection SCAD is a rare , different entity , enjoys a popular space in the patho-physiology of CAD.
No signs for aortic dissection or pulmonary embolus. --"Results were discussed with the ordering physician. A CT Coronary angiogram was ordered. Here are the results: --Minimally obstructive coronary artery disease. --LAD LAD plaque with 0-25 percent stenosis. CAD-RADS category 1. --No
SMART 4 ( NCT04722250 ) studied patients with severe aortic stenosis and a small aortic annulus who underwent transcatheter aortic valve replacement (TAVR). The primary endpoint consisted of a composite of all-cause mortality, MI, stroke, coronary revascularization, or hospitalization for unstable angina.
1,2 ASCVD causes or contributes to conditions that include coronary artery disease (CAD), cerebrovascular disease, and peripheral vascular disease (inclusive of aortic aneurysm).3 The benefit was most significant in reducing the incidence of stroke and angina requiring revascularization.35 4 In the U.S. 12 Importantly, colchicine, 0.5
Beware crescendo angina in patient with known CAD ST Elevation in aVR Case 7. baseline LVH, demand ischemia secondary to respiratory failure, aortic stenosis, hemorrhagic shock). And thus it is a hybrid of de Winter's T-waves and Diffuse subendocardial ischemia. Another left main occlusion, but this one shows subendocardial ischemia.
If LV contraction interferes with coronary blood flow, a patient with severe LV dysfunction gains some advantage as systolic blood flow can happen more easily, and myocardium is perfused better, provided his aortic systolic pressure not too low enough. How common is angina in DCM ? Angina in DCM is an exception despite elevated LVEDP.
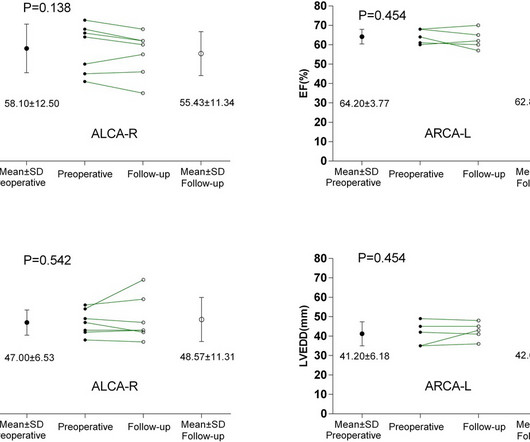
BackgroundAnomalous aortic origin of a coronary artery (AAOCA) is associated with an increased risk of myocardial ischemia and sudden cardiac death. The incidence of postoperative cardiac-type symptoms (angina, syncope or dyspnea) was higher in ALCA-R patients compared to ARCA-L patients.
Larger shunt volume means less blood exiting the left ventricle through the aortic valve and lower cardiac output. The pressure gradient in this case was significant indicating that the defect is rather small. The larger the size of the defect the larger the shunt.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content