This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
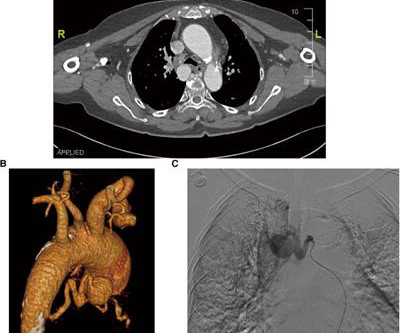
Bronchial artery aneurysm (BAA) is a rare and fatal condition that requires immediate treatment. In the present case, a 76-year-old hypertensive woman was admitted with dizziness and diagnosed with an unruptured bronchial artery aneurysm, which was treated by transcatheter arterial embolization and aortic stent-graft.
It is of an elderly woman who complained of shortness of breath and had a recent stent placed. LV aneurysm has QS-waves, so this couldn't be LV aneurysm, right? RBBB makes it mandatory that there are R'-waves even in the presence of LV aneurysm. Also, we know the patient had a stent. What do you think?
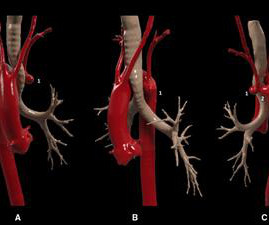
In this case, we present a symptomatic patient with a Kommerell's diverticulum and a left aberrant subclavian artery complicated by proximal stenosis and poststenotic aneurysm.
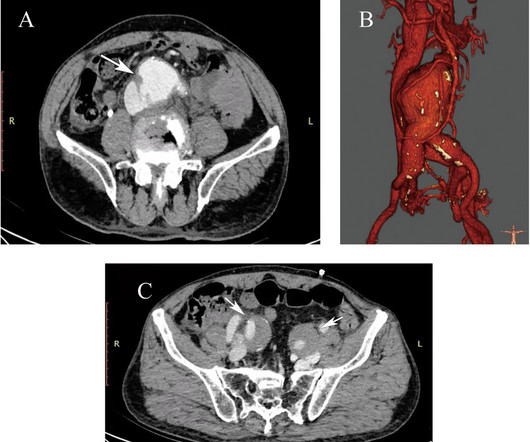
BackgroundAorto-caval fistula is a rare complication of abdominal aortic aneurysms that can occur spontaneously, iatrogenically, or traumatically, associated with high morbidity and mortality. Computed tomography angiography revealed an aorto-caval fistula complicating infrarenal abdominal aortic aneurysm.
BackgroundAbdominal aortic aneurysm (AAA) is a localized bulge of the abdominal aorta, which mainly manifests as a pulsatile mass in the abdomen. Once an abdominal aortic aneurysm ruptures, the patient's life is seriously endangered. Surgery is the preferred treatment for abdominal aortic aneurysm.
IntroductionThe accuracy of fenestrations in stent grafts for complex aortic aneurysms and dissections can be significantly improved using three-dimensional (3D)-printed phantoms. Standardization is enhanced by using artificial intelligence (AI) for image pre-processing before 3D printing.
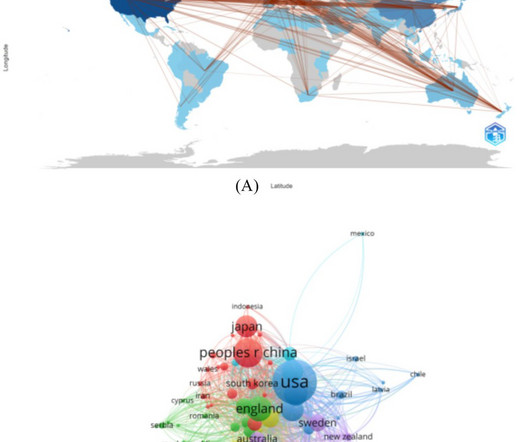
Objective This study aims to review the application of deep learning techniques in the imaging diagnosis and treatment of aortic aneurysm (AA), focusing on screening, diagnosis, lesion segmentation, surgical assistance, and prognosis prediction.
There are QS-waves in V1-V3 suggesting old anterior MI with persistent ST Elevation (LV aneurysm morphology), but I have written a couple papers showing that in LV aneurysm, the T-wave is not > 0.36 T/QRS Amplitude Best Distinguishes Acute Anterior MI from Anterior Left Ventricular Aneurysm. LV Aneurysm vs New Infarction?
(Gore) announced recent FDA approval of a lower profile GORE VIABAHN VBX Balloon Expandable Endoprosthesis ( VBX Stent Graft ). 1-3 "Our team is pleased to be the first commercial implanter of the new lower profile VBX Stent Graft," said Darren Schneider , M.D., No changes to the stent design were made to achieve the lower profile.
Anastomotic aneurysms present as a life-threatening emergency after descending aortic replacement for aortic dissection. Thoracic endovascular aneurysm repair (TEVAR) has been performed since the early 2000s f.
BackgroundThe risk of limb graft occlusion (LGO) after endovascular aneurysm repair (EVAR) is increased by severe tortuosity of the iliac artery. In total, 50 individuals were included in group A, while 107 were in group B.
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. So it would be wise to look at the pre-discharge ECG, which was available: There are Q-waves and ST elevation on this pre-discharge (post-stent) ECG. He had no chest pain.
Introduction:Surpass Evolve (SE) is an updated flow diverter stent. While shown to be effective and safe for treating intracranial aneurysms (IA), blood flow analysis is still limited. Stroke, Volume 56, Issue Suppl_1 , Page AWP258-AWP258, February 1, 2025. For each case, a SE device measuring 3.25 respectively).
Objective:Recanalized aneurysms may still recanalize despite a second coiling to prevent rupture. Factors related to recanalization following a second coiling for recanalized aneurysms have not yet been fully explored. months), 72 (38.3%) of 188 recanalized aneurysms developed major recanalization.
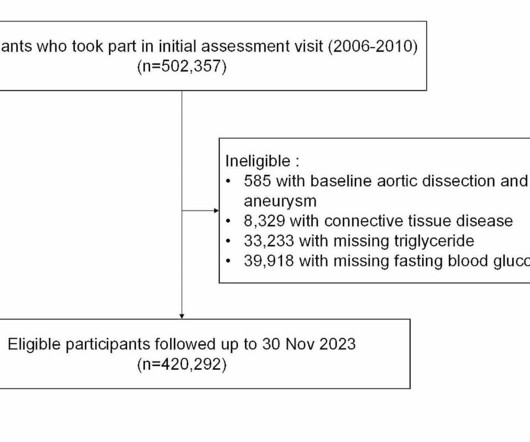
Triglyceride-glucose (TyG) index is an emerging surrogate indicator of insulin resistance, which has been demonstrated as a risk factor for various cardiovascular diseases including coronary syndrome, in-stent.
Although diagnostic of MI, it is highly suspicious for " Old inferior MI with persistent ST Elevation" or "inferior aneurysm morphology" because of the well-formed Q-waves and the flat T-waves. To repeat: in contrast, anterior aneurysm is much more easily distinguished from acute MI due to the QS-waves.
years) underwent surgery for unruptured anterior communicating artery aneurysms in our hospital between January 2018 and January 2023.ResultsThe ResultsThe mean aneurysm dome size was 5.29 mm (2–22 mm), and the mean aneurysm neck size was 3.2 12; ATLAS, 14). Follow‐up was performed in 55 patients, averaging 29.5
IntroductionBasilar‐tip aneurysm (BTA) is the most common aneurysm found in the posterior circulation, representing 5–8% of total intracranial aneurysms. For ruptured aneurysms, Adjuvant therapy (BAC or SAC) was used to treat larger dimension aneurysms compared to CE (p = 0.046). vs. 10.7%).
IntroductionFlow diverters (FD) are stent‐type devices that enable the exclusion of intracranial aneurysms in clinical scenarios where coil‐type devices exhibit high failure rates. Adults older than 18 with non‐ruptured intracranial aneurysms were included. years (±13.3). years (±13.3).
IntroductionIntracranial aneurysms, both ruptured and unruptured, pose a significant risk to the general population. Cases of unruptured intracranial aneurysms (UIA) are estimated to affect roughly 3% of the general population and aneurysmal subarachnoid hemorrhage (aSAH) have an incidence of 8 to 9 people per 100,000.
Ruptured aneurysmal subarachnoid hemorrhage accounted for 15.7% (8/51) of all patients. The most common aneurysm location in the present study was MCA bifurcation (52.9%). The median maximal aneurysm diameter was 6.9mm, while the median neck size was 4.4mm. Retreatment was required in 1 aneurysm.
IntroductionFlow diversion (FD) is commonly used for the treatment of aneurysms involving the ophthalmic segment of the carotid artery (COA). The origin of the ophthalmic artery (OA) in relation to the aneurysm sac can affect recurrence and complications. directly from the aneurysm fundus, B. aneurysm neck, C.
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. The patient had a history of ‘NSTEMI’ a decade prior, with an RCA stent. Does this change your interpretation?
Background and Purpose:The flow diverter (FD) has dramatically improved the treatment outcome of large / giant internal carotid artery (IC) aneurysms. Stroke, Volume 55, Issue Suppl_1 , Page ATP151-ATP151, February 1, 2024. However, it is difficult to predict the treatment outcome of FD just after the treatment.
Previous medical interventions included a spectrum of procedures, including catheter-directed thrombectomy for popliteal artery aneurysms with thrombosis, vascular bypass grafting for cerebral-anterior communicating artery aneurysms and arch replacement and stent implantation for aortic dissecting aneurysms.
BACKGROUNDThe optimal endovascular approach for acutely ruptured wide‐neck intracranial aneurysms remains uncertain, and the use of stent‐assisted coiling or flow diversion is controversial due to antiplatelet therapy requirements and potential risks. Stroke: Vascular and Interventional Neurology, Ahead of Print. versus BAC: 2.8%;P=
Introduction:The management of wide-necked internal carotid artery (ICA) aneurysms is technically challenging with established endovascular and microsurgical techniques that are limited by the associated morbidity and/or recurrence. Median aneurysm and neck size were 5.8 mm (IQR: 4.0-7.5) At a median 10.1 months (IQR: 6.3-12.6),
IntroductionThe optimal endovascular approach for wide‐neck intracranial aneurysms (IAs) during the acute phase of bleeding remains uncertain, and the use of stent‐assisted coiling or flow diversion is controversial due to antiplatelet therapy requirements and potential risks (1, 2).
5 ICSS‐ MRI study (International Carotid Stenting Study Magnetic Resonance Imaging Study), indicated that patients with periprocedural hemodynamic depression had decreased cerebral blood flow and increased the risk of new lesions in imaging.6 This is secondary to delayed postoperative cerebral ischemia and infarction caused by vasospasm.7
IntroductionIndications for flow diversion for the treatment of cerebral aneurysms have increased remarkably in recent years.1 1 This has been particularly useful for aneurysms that are difficult to treat via endosaccular or open approaches, such as pseudoaneurysms.2
Furthermore, it aids in planning and conducting safe aortic intervention and assists in deciding on single- or two-staged stent graft procedures. It underscores the value of preoperative CT councils and provides crucial information for interpreting the results.
However, old MI w/aneurysm morphology (persistent ST-Elevation) can look just like this. While this may be change that is reciprocal to an Acute/Subacute Inferior STEMI, the problem is that LV aneurysm may also manifest with this reciprocal change. Old MI w/Aneurysm will show moderate ST Elevation, as seen here.
It can provide intraluminal fly-through and clipping-plane views which help endovascular assessment of stents, aneurysms, vessel wall irregularities and calcification. The dataset could even be used to generate 3D-printed models of congenital heart disease [2]. Reference Kang SL, Armstrong A, Krings G, Benson L.
Of the 32 patients, 9(28.1%) had dissection with diagnostic angiograms, 6(18.8%) endovascular thrombectomy, 15(46.9%) aneurysm treatment, and 2(6.3%) angioplasty with or without stenting. Only 4(12.5%) were treated with hyperacute stenting. One patient was symptomatic with neck pain.
The workshop included 3 stations: basic equipment orientation, overview of endovascular techniques for ischemic stroke, and an intracranial aneurysm treatment model treatment station. Participants had an opportunity to rotate through each station at least once. Participants were asked to voluntarily provide feedback via electronic survey.
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. The patient underwent successful placement of one drug eluting stent with restoration of TIMI 3 flow.
All three lesions had TIMI 2 flow prior to stenting. This is an RAO cranial projection of the left coronary vessels after thrombectomy and stenting. The LV aneurysm morphology persists. Here, the mid LAD (blue arrow) and the ostial first diagonal (green arrow) stenoses are better visualized. This is the RAO caudal projection.
It was opened and stented. This may be permanent and may be associated with echocardiographic dyskinesis (aneurysm). LV aneurysm is common in completed, full thickness (transmural) MI, which is what we have here. LV aneurysm puts them at risk for a mural thrombus, which puts them at risk for embolism, especially embolic stroke.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. The EKG is diagnostic of acute inferior, posterior, and lateral OMI superimposed on “LV aneurysm” morphology. It was stented. He wrote most of it and I (Smith) edited.
Persistent ST elevation 3 days after a nearly transmural MI portends possible LV aneurysm. It is very unlikely to be LV aneurysm morphology when the ST elevation is so high and the T-Wave inversion is so deep. An open 90% LAD was stented. This 42 yo diabetic male presented with cough and foot pain. The LAD has reperfused early.
Also a h/o LV aneurysm with thrombus, on anticoagulation, as well as a dual chamber pacemaker. It was opened and stented with resulting TIMI-3 (normal) flow. The stent to LCX is patent. Aneurysm of the mid-portion of the lateral and inferolateral wall. They called 911. On arrival, the BP was 60/30.
hours after that first diagnostic ECG) : Mid-LAD culprit lesion, 99% stenosis, no pre-intervention TIMI flow available, but described as "severe subtotal lesion", which was stented with reported TIMI 3 flow resulting. Another lesion in the proximal LAD with 80% stenosis was stented as well. Culprit lesion was reduced to 0% and stented.
Studies reporting results of patients who underwent diagnostic angiograms, endovascular management of acute stroke, aneurysm repair, and carotid or vertebral stenting were included. Randomized clinical trials (RCT) and observational studies that compared TRA and TFA were included.
This unique case highlights the diagnostic and therapeutic challenges of a patient with multiple vascular risk factors who suffered from strokes secondary to BHS.MethodsA 79‐year‐old man with a past medical history of peripheral artery disease, abdominal aortic aneurysm, myocardial infarction with drug eluding stents (on dual antiplatelet therapy (DAPT)), (..)
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.









































Let's personalize your content