This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
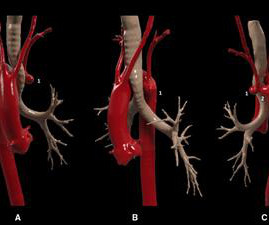
In this case, we present a symptomatic patient with a Kommerell's diverticulum and a left aberrant subclavian artery complicated by proximal stenosis and poststenotic aneurysm.
Although diagnostic of MI, it is highly suspicious for " Old inferior MI with persistent ST Elevation" or "inferior aneurysm morphology" because of the well-formed Q-waves and the flat T-waves. To repeat: in contrast, anterior aneurysm is much more easily distinguished from acute MI due to the QS-waves.
years) underwent surgery for unruptured anterior communicating artery aneurysms in our hospital between January 2018 and January 2023.ResultsThe ResultsThe mean aneurysm dome size was 5.29 mm (2–22 mm), and the mean aneurysm neck size was 3.2 12; ATLAS, 14). Postoperative thrombotic complications were observed in 1 patient.
Old ‘NSTEMI’ A history of coronary artery disease and a stent to the same territory further increases pre-test likelihood of acute coronary occlusion, including in-stent thrombosis. The patient had a history of ‘NSTEMI’ a decade prior, with an RCA stent. Does this change your interpretation?
Introduction:The management of wide-necked internal carotid artery (ICA) aneurysms is technically challenging with established endovascular and microsurgical techniques that are limited by the associated morbidity and/or recurrence. Median aneurysm and neck size were 5.8 mm (IQR: 4.0-7.5) At a median 10.1 months (IQR: 6.3-12.6),
The red arrow shows a roughly 80% stenosis of the proximal LAD. The blue arrow shows another stenosis of the LAD distal to the first diagonal branch of about 99%. The green arrow shows a 95% stenosis of the ostium of the first diagonal branch. All three lesions had TIMI 2 flow prior to stenting.
However, CTA head and neck 4 days later demonstrated 90 percent stenosis of the mid left V2 at the C3‐4 level and a 75‐90 percent stenosis of the left mid V2 segment at the C5‐6 level (hard and soft plaque in these areas). He also had moderate stenosis of the right V4 segment.
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. The EKG is diagnostic of acute inferior, posterior, and lateral OMI superimposed on “LV aneurysm” morphology. Angiography revealed a 30% nonobstructive stenosis of the mid LAD.
hours after that first diagnostic ECG) : Mid-LAD culprit lesion, 99% stenosis, no pre-intervention TIMI flow available, but described as "severe subtotal lesion", which was stented with reported TIMI 3 flow resulting. Another lesion in the proximal LAD with 80% stenosis was stented as well. Angiogram @ 1830 (3.3
Submitted and written by Alex Bracey with edits by Pendell Meyers and Steve Smith Case A 50ish year old man with a history of CAD w/ prior LAD MI s/p LAD stenting presented to the ED with chest pain similar to his prior MI, but worse. The patient underwent successful placement of one drug eluting stent with restoration of TIMI 3 flow.
Also a h/o LV aneurysm with thrombus, on anticoagulation, as well as a dual chamber pacemaker. It was opened and stented with resulting TIMI-3 (normal) flow. The stent to LCX is patent. OM1 is occluded and OM2 has 60% stenosis. Her RCA is a medium caliber vessel with tandem, at least moderate stenosis in the mid segment.
They found an acute lesion of the LAD at the site of the prior stents, including 70% proximal LAD lesion and 95% mid-LAD stenosis with TIMI 3 flow at the time of cath. The LAD lesion was acute and required 3 stents to restore flow. They took him almost immediately for catheterization. Similar findings.
A middle-aged male with h/o CAD and stents presented with typical chest pressure. An elderly patient with a ruptured abdominal aortic aneurysm: Formal ECG Interpretation (final read in the chart!) : "Inferior ST elevation, lead III, with reciprocal ST depression in aVL." This is a very common misread. What do you think?
Introduction:Although flow diverters (FD) are a long-established treatment-option for brain aneurysms, the evidence of data associated with therapy success is still based on relatively small heterogeneous studies. Median diameter and neck width of aneurysms were 7.2 91.7% (719) of aneurysms were saccular. mm (IQR, 5-11) and 6.5
No thoracic aortic hematoma, aneurysm or dissection. First obtuse marginal also had an 80% stenosis and was stented. Patient states pain improved on ambulance ride over after receiving 325 mg Aspirin and nitroglycerin, with pain down to 2/10. CT Angio Chest IMPRESSION 1. No pulmonary embolism is identified.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.




















Let's personalize your content