This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
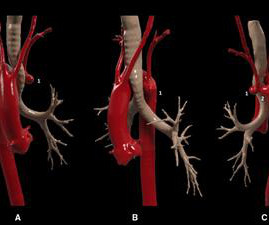
In this case, we present a symptomatic patient with a Kommerell's diverticulum and a left aberrant subclavian artery complicated by proximal stenosis and poststenotic aneurysm.
Background Bicuspid aortic valve (BAV) is the most common congenital heart defect in adults, often leading to complications such as thoracic aortic aneurysms and aortic stenosis. While BAV is frequently associated with 22q11.2
We present a case of a 22-month-old boy with a hypokinetic and thin-walled aneurysm of the left ventricle apex. Cardiac magnetic resonance imaging revealed an akinetic aneurysm of the LV apex with a full-wall ischemic scar. Determining the origin of the aneurysm is challenging.
Kawasaki disease (KD), an acute self-limited febrile illness that primarily affects children <5 years old, is the leading cause of acquired heart disease in developed countries, with the potential of leading to coronary artery dilation and coronary artery aneurysms in 25% of untreated patients.
years) underwent surgery for unruptured anterior communicating artery aneurysms in our hospital between January 2018 and January 2023.ResultsThe ResultsThe mean aneurysm dome size was 5.29 mm (2–22 mm), and the mean aneurysm neck size was 3.2 12; ATLAS, 14). Postoperative thrombotic complications were observed in 1 patient.
Introduction:Medical treatment of internal carotid artery stenosis consists of treatment of underlying conditions such as hypertension, dyslipidemia, and diabetes mellitus, as well as antiplatelet therapy. Similarly, cerebral aneurysms are known to progress due to hemodynamic effects.
Introduction18‐36% of all intracranial aneurysms are middle cerebral artery(MCA) bifurcation aneurysms. 1) MCA bifurcation aneurysms have been historically challenging to treat endovascularly given they often have complex morphology and wide necks. Final angiography revealed complete occlusion of the aneurysm.
Introduction:The management of wide-necked internal carotid artery (ICA) aneurysms is technically challenging with established endovascular and microsurgical techniques that are limited by the associated morbidity and/or recurrence. Median aneurysm and neck size were 5.8 mm (IQR: 4.0-7.5) At a median 10.1 months (IQR: 6.3-12.6),
Eagle looks at a prospective multicenter cohort study that examined early and late aortic-related mortality and rupture after fenestrated-branched endovascular aortic repair of thoracoabdominal aortic aneurysms.
Blood lipids such as cholesterol and triglycerides are causal risk factors for coronary heart disease as well as several other types of cardiovascular disease , such as aortic stenosis). Smoking is a prevalent risk factor among people who have an abdominal aortic aneurysm.
We performed coronary angiography for the patient with ECMO support, indicating that the patient had an 80% critical stenosis of the left main coronary artery and an 80%–90% stenosis in the middle section of the left anterior descending artery with an aneurysm.
Smith : Old inferior MI with persistent ST Elevation ("inferior aneurysm") has well-formed Q-waves. In inferior aneurysm, we usually see QR-waves, whereas for anterior aneurysm, we see QS-waves (no R- or r-wave at all!). The patient had a history of ‘NSTEMI’ a decade prior, with an RCA stent.
Although diagnostic of MI, it is highly suspicious for " Old inferior MI with persistent ST Elevation" or "inferior aneurysm morphology" because of the well-formed Q-waves and the flat T-waves. To repeat: in contrast, anterior aneurysm is much more easily distinguished from acute MI due to the QS-waves.
The old ECG has a Q-wave with persistent ST elevation in lead III, and some reciprocal ST depression (typical for aneurysm morphology). This is "Persistent ST elevation after previous MI" or "LV aneurysm morphology". LV aneurysm is very different for inferior vs. anterior MI. The patient had a critical LAD stenosis.
However, CTA head and neck 4 days later demonstrated 90 percent stenosis of the mid left V2 at the C3‐4 level and a 75‐90 percent stenosis of the left mid V2 segment at the C5‐6 level (hard and soft plaque in these areas). He also had moderate stenosis of the right V4 segment.
Coronary angiography revealed a tortuous and extremely aneurysmal RCA, as well as multivessel coronary artery disease (mvCAD) involving LAD, D1, LCx, OM1. Notably, the LAD had multiple aneurysmal segments and areas of eccentric stenosis upto 90%.Multislice
The red arrow shows a roughly 80% stenosis of the proximal LAD. The blue arrow shows another stenosis of the LAD distal to the first diagonal branch of about 99%. The green arrow shows a 95% stenosis of the ostium of the first diagonal branch. The LV aneurysm morphology persists. This is the RAO caudal projection.
Most cases were performed in an emergency condition, such as ruptured VA dissecting aneurysm (73 cases [70.2%]). The remaining image change was contralateral VA stenosis after VA PAO. years old; men, 73 [70.2%] cases; 95 [91.3%] VA PAO cases) from 8 centers. PAO was successful in all cases.
Transcatheter Aortic Valve Replacement (TAVR): TAVR is performed for patients with severe cases of aortic stenosis, which is the thickening of the aortic valve. It involves a metal sent, which is inserted into the aneurysm and aims to replace the damaged part of the aorta.
carotid artery stenosis and unruptured cerebral aneurysm), abnormal symptoms or pathological findings (e.g. Among 339 (7%) people, there were 351 ED presentations within the 7 days before stroke and among 676 (13.78%) people, there were 765 ED presentations in the 30 days before stroke. migraine) and respiratory diseases (Table 1).
While certain angioarchitectural features, such as aneurysms, deep venous drainage, a single draining vein, venous outflow stenosis, or small nidus size, increase hemorrhage risk, they do not fully predict it. Background:Pediatric brain arteriovenous malformation (bAVM) patients often present with intracranial hemorrhage.
BackgroundSupravalvar aortic stenosis (SVAS) is a characteristic feature of Williams–Beuren syndrome (WBS). Journal of the American Heart Association, Ahead of Print. Its severity varies: ~20% of people with Williams–Beuren syndrome have SVAS requiring surgical intervention, whereas ~35% have no appreciable SVAS.
The EKG is diagnostic of acute inferior, posterior, and lateral OMI superimposed on “LV aneurysm” morphology. Angiography revealed a 30% nonobstructive stenosis of the mid LAD. There was a 70% culprit stenosis of the first obtuse marginal branch in a right dominant system. Patient 2 , EKG 1: What do you think?
It showed a 99% stenosis in the RCA, and proximal to a posterolateral branch. A coronary aneurysm was found. Some of these MIs in young people are due to anomolies: aneurysm from a disorder known to be associated with coronary aneurysms (left out to maintain anonymity) in this case. A second troponin returned at 1.71
Early onset symptoms of the disease were defined as moderate or severe aortic stenosis or aortic regurgitation, a large thoracic aortic aneurysm, needing to have aortic surgery, or aortic dissection. Researchers aimed to identify genetic variants that may lead to an increased risk of the disease in young adults.
Also a h/o LV aneurysm with thrombus, on anticoagulation, as well as a dual chamber pacemaker. OM1 is occluded and OM2 has 60% stenosis. Her RCA is a medium caliber vessel with tandem, at least moderate stenosis in the mid segment. Aneurysm of the mid-portion of the lateral and inferolateral wall. They called 911.
Cerebral angiogram showed diffuse multifocal narrowing with a ‘beads‐on‐a‐string’ appearance of the cerebral vasculature and no aneurysms (Figure 3). Brain MRA 3 months after discharge showed no areas of cerebrovascular focal stenosis (Figure 4). Thrive patch contains undisclosed amounts of sympathomimetics and vasoactive compounds.
hours after that first diagnostic ECG) : Mid-LAD culprit lesion, 99% stenosis, no pre-intervention TIMI flow available, but described as "severe subtotal lesion", which was stented with reported TIMI 3 flow resulting. Another lesion in the proximal LAD with 80% stenosis was stented as well. Culprit is 100% stenosis in the Proximal LAD.
When there is associated mitral stenosis, the colour Doppler jet of mitral flow merges with that of aortic regurgitation in the left ventricle as both occur in diastole. Eccentric aortic regurgitation has been reported in ascending aortic aneurysm. m/sec, indicating the absence of any associated aortic stenosis.
Here are the images from the cardiac cath: Mid to distal-LAD in-stent stenosis with 100% occlusion and TIMI flow 0 LAD post-DES placement with TIMI 3 flow The amount of territory supplied by this vessel becomes obvious here (and goes on for a few more frames below this still). No further echocardiograms were available after cath.
They found an acute lesion of the LAD at the site of the prior stents, including 70% proximal LAD lesion and 95% mid-LAD stenosis with TIMI 3 flow at the time of cath. In Dr. Smith's experience one must wait at least 2 weeks to find out if this electrical LVA morphology will resolve, and whether it will be accompanied by anatomic aneurysm.
An elderly patient with a ruptured abdominal aortic aneurysm: Formal ECG Interpretation (final read in the chart!) : "Inferior ST elevation, lead III, with reciprocal ST depression in aVL." Is there likely to be fixed coronary stenosis that led to demand ischemia during pneumonia? --Was What do you think? Does he need a stress test? --Is
The patient's heart had significant recovery: Echo : Estimated LVEF 32%, apical wall motion abnormality with diastolic distortion (LV aneurysm), suggestive of old MI. distal stenosis or occluded small branches), and 3) nonischemic causes for myocyte injury (e.g., It was uncertain whether this represented: 1. myocarditis).
Note that this obvious STEMI does not have 100% stenosis at the time of cath. It showed a mid LAD culprit with 95% with no pre intervention timi flow listed. PCI was performed, with TIMI 3 flow after the intervention. A significant portion of obvious STEMIs have TIMI 3 flow upon rapid angiogram. hours earlier?
Repeat ECG at 1624 (shortly before cath): QS waves now present in V2-V3, with slight STE, showing the pattern of left ventricular aneurysm morphology. Upon arrival to the PCI center, the repeat troponin returned at 13,962 ng/L. Chest pain is documented as ongoing.
Introduction:Although flow diverters (FD) are a long-established treatment-option for brain aneurysms, the evidence of data associated with therapy success is still based on relatively small heterogeneous studies. Median diameter and neck width of aneurysms were 7.2 91.7% (719) of aneurysms were saccular. mm (IQR, 5-11) and 6.5
Meschia’s lecture, “Asymptomatic Carotid Stenosis: Current and Future Considerations,” will be presented Feb. Globus New Investigator Award in Stroke awardee, is a postdoctoral fellow at Barrow Aneurysm & AVM Research Center (BARRC) at the Barrow Neurological Institute in Phoenix. Chimowitz, M.B., Ch.B. , the recipient of the Ralph L.
Transvenous, external carotid, and strokerelated interventions were excluded.RESULTSOf 62 total interventions with the Armadillo catheter, 58 procedures (53/58 [91.4%] for aneurysms, 3/58 [5.6%] for arteriovenous malformations, and 2/58 [3.4%] for intracranial stenosis) in 55 patients (mean age, 57.2 standrad deviation (SD), 12.4]
The protein model also improved the prediction of other outcomes, including ASCVD (cstatistic +0.035), myocardial infarction (+0.023), stroke (+0.024), aortic stenosis (+0.015), heart failure (+0.060), abdominal aortic aneurysm (+0.024), and dementia (+0.068).CONCLUSIONS:Measurement
Look for Vascular Etiology -- think of these while doing H and P: --Bleeding: ruptured AAA, GI bleed, ruptured ectopic pregnancy, other spontaneous bleed such as mesenteric aneurysms. Aortic Dissection, Valvular (especially Aortic Stenosis), Tamponade. heart auscultation (aortic stenosis); c. orthostatic vitals b.
There are no Q-waves to suggest old inferior MI, or inferior aneurysm as the etiology of the ST Elevation. Smith : "decompensation" of aortic stenosis might have initiated this entire cascade. What "initiates" the aortic stenosis cascade? The scan showed a bicuspid aortic valve with severe stenosis and coronary artery disease.
No thoracic aortic hematoma, aneurysm or dissection. First obtuse marginal also had an 80% stenosis and was stented. Patient states pain improved on ambulance ride over after receiving 325 mg Aspirin and nitroglycerin, with pain down to 2/10. CT Angio Chest IMPRESSION 1. No pulmonary embolism is identified.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content