This site uses cookies to improve your experience. To help us insure we adhere to various privacy regulations, please select your country/region of residence. If you do not select a country, we will assume you are from the United States. Select your Cookie Settings or view our Privacy Policy and Terms of Use.
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Used for the proper function of the website
Used for monitoring website traffic and interactions
Cookie Settings
Cookies and similar technologies are used on this website for proper function of the website, for tracking performance analytics and for marketing purposes. We and some of our third-party providers may use cookie data for various purposes. Please review the cookie settings below and choose your preference.
Strictly Necessary: Used for the proper function of the website
Performance/Analytics: Used for monitoring website traffic and interactions
There were many comments that it was too late for thrombolytics or that this signified an LV aneurysm, not acute MI. See my formula for differentiating anterior LV aneurysm (that is to say, persistent ST elevation after old MI) from acute anterior STEMI. Both support acute anterior STEMI. It is not chronic. 3.0 = 0.50
A male in his 40's who had been discharged 6 hours prior after stenting of an inferoposterior STEMI had sudden severe SOB at home 2 hours prior to calling 911. Is this acute STEMI? Is this an acute STEMI? -- Unlikely! He had no chest pain. Medications were aspirin, clopidogrel, metoprolol, and simvastatin.
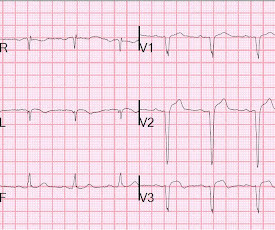
STEMI – Anterior Wall ECG shows ST elevation myocardial infarction of anterior wall. Similar changes may also be noted in left ventricular aneurysm after a myocardial infarction as the ST segment may remain elevated when there is a dyskinetic segment. T wave inversions are seen in leads I and aVL as well.
He was rushed by residents into our critical care room with a diagnosis of STEMI, and they handed me this ECG: There is sinus tachycardia with ST elevation in II, III, and aVF, as well as V4-V6. At first glance, it seems the patient is having a STEMI. ACS and STEMI generally do not cause tachycardia unless there is cardiogenic shock.
Smith : Old inferior MI with persistent ST Elevation ("inferior aneurysm") has well-formed Q-waves. In inferior aneurysm, we usually see QR-waves, whereas for anterior aneurysm, we see QS-waves (no R- or r-wave at all!). So this NSTEMI was likely a STEMI(-)OMI with delayed reperfusion. Deutch et al.
He has a history of STEMI and heart failure. The only alternative is old inferior MI with persistent ST-Elevation, or inferior aneurysm morphology. Inferior Aneurysm morphology is incredibly hard to differentiate from Acute OMI, but you should suspect it whenever there are well-formed inferior Q-waves. He had a prehospital ECG.
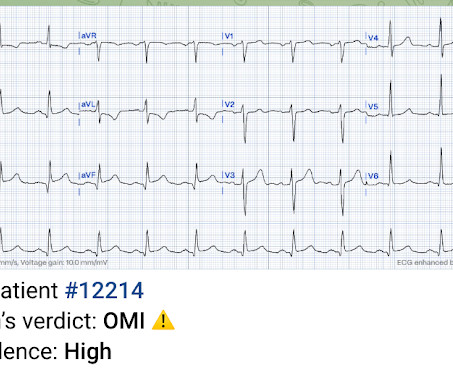
IMPRESSION: In this patient who presents with severe, new-onset CP — today's ECG is diagnostic of an extensive, ongoing antero-lateral STEMI. ECG Blog #193 — Reviews the basics for predicting the " culprit " artery ( as well as reviewing why the term "STEMI" — should be replaced by "OMI" = O cclusion-based MI ).
This is a 45 yo male who had an inferior STEMI 6 months prior, was found to have severe LAD and left main disease, and was supposed to be set up for CABG a few weeks later, but did not follow up. But it could be anterior STEMI. 40% of anterior STEMI has upward concavity in all of leads V2-V6. is likely anterior STEMI).
These elevations meet STEMI criteria ( ≥ 1mm in 2 contiguous leads). However, old MI w/aneurysm morphology (persistent ST-Elevation) can look just like this. While this may be change that is reciprocal to an Acute/Subacute Inferior STEMI, the problem is that LV aneurysm may also manifest with this reciprocal change.
Echo on the day after admission showed EF of 30-35% and antero-apical wall akinesis with an LV thrombus [these frequently form in complete or near complete (no early reperfusion) anterior STEMI because of akinesis/stasis] 2 more days later, this was recorded: ST elevation is still present. Cath showed a 95% LAD with flow. This was recorded 2.5
Only very slight STE which does not meet STEMI criteria at this time. I am immediately worried that this OMI will not be understood, for many reasons including lack of sufficient STE for STEMI criteria, as well as the common misunderstanding of "no reciprocal findings" which is very common with this particular pattern. 6.5 = 0.38.
would require the ST/S ratio to be 25% for diagnosis of STEMI in LVH. The physician was concerned about STEMI, but also worried that she was overreacting, with the potential that LVH was producing a "STEMI-mimic." Can you diagnose an ACO (STEMI) when you also have LVH? Is LVH like left ventricular aneurysm?
A prehospital “STEMI” activation was called on a 75 year old male ( Patient 1 ) with a history of hyperlipidemia and LAD and Cx OMI with stent placement. The EKG is diagnostic of acute inferior, posterior, and lateral OMI superimposed on “LV aneurysm” morphology. The prehospital ECG of Patient #1 — showed an obvious acute STEMI.
The prehospital and ED computer interpretation was inferior STEMI: There’s normal sinus rhythm, first degree AV block and RBBB, normal axis and normal voltages. The paramedic notes called STEMI into question: “EMS disagree with monitor for STEMI callout. Vitals were normal except for oxygen saturation of 94%. Vitals were normal.
Diagnosis: There are Q-waves, ST elevation, and hyperacute T-waves in V2 and V3, diagnostic of acute LAD occlusion (STEMI). Sometimes you will find an obvious STEMI. This may resolve over a couple weeks; if it does not, then he is at high risk of developing an LV aneurysm, or diastolic dysfunction of the anterior wall.
How can one distinguish MI vs LV aneurysm on ECG? 9 patients presented with potentially ischemic symptoms and Q-waves. Which had Occlusion MI? What is the differential diagnosis of Q-waves? The post ECG Cases 14: Q-wave and Occlusion MI appeared first on Emergency Medicine Cases.
STE occurs primarily in viable ischemic myocardium; persistent STE after completed infarction is ominous and portends development of an aneurysm. But it does not meet STEMI criteria and it was not initially recognized. Whereas most STEMI(-) OMI is acute, this one might have had STE at its onset, or earlier in its course.
This may be permanent and may be associated with echocardiographic dyskinesis (aneurysm). LV aneurysm is common in completed, full thickness (transmural) MI, which is what we have here. It is uncommon in the age of reperfusion therapy, as most STEMI get treated reasonably early, before transmural infarct.
We have found in our study comparing inferior STEMI (manuscript in preparation) to inferior early repol several distinguishing characteristics. A coronary aneurysm was found. And young women have worse outcomes than other groups with STEMI because of the tendency to say, "Nah, couldn't be!" A second troponin returned at 1.71
But the well-formed Q-wave and the presence of a normal T-wave in inferior leads led me to believe this was Old Inferior MI with persistent ST Elevation, otherwise known as inferior LV aneurysm. Anterior LV aneurysm is much easier to recognize because the Q-wave is usually a QS-wave (no R-wave at all), in at least one lead.
Barely any STE, and thus not meeting STEMI criteria. Annals of Emergency Medicine Cardiology was called to evaluate the patient immediately for emergent cath, but they stated that the ECG did not meet STEMI criteria and elected to wait for further information before proceeding with cath. He was given 6mg IV morphine for ongoing pain.
Despite ongoing chest discomfort and an uptrending troponin, he never meets STEMI criteria. The full thickness infarction with LV aneurysm morphology places him at a higher risk for short and long term complications (e.g., Free wall rupture, VSD, Dresslers Syndrome, chronic CHF, anatomic LV aneurysm, LV thrombus, stroke, etc).
The Queen of Hearts correctly says: Smith : Why is this ECG which manifests so much ST Elevation NOT a STEMI (even if it were a 60 year old with chest pain)? Physician interpretation: "No STEMI." Physician: "No STEMI." Cardiologist interpretation: "Technically does not meet STEMI criteria but concerning for ischemia."
Also a h/o LV aneurysm with thrombus, on anticoagulation, as well as a dual chamber pacemaker. Aneurysm of the mid-portion of the lateral and inferolateral wall. Marked acute STEMI changes in no less than 4 lateral leads. They called 911. On arrival, the BP was 60/30. See the outpouching at the bottom of the image.
This is a troponin I level that is almost exclusively seen in STEMI. The patient's heart had significant recovery: Echo : Estimated LVEF 32%, apical wall motion abnormality with diastolic distortion (LV aneurysm), suggestive of old MI. So this is either a case of MINOCA, or a case of Type II STEMI. Troponin I rose to 44.1
Old MI with persistent ST Elevation (LV aneurysm morphology) can look like acute MI 2. Not all anterior LV aneurysm has a QS-wave. Dyspnea, Right Bundle Branch block, and ST elevation Here are two more cases where the differential diagnosis is acute OMI vs. LV aneurysm: Is this acute STEMI? LV Aneurysm?
The only time you see this without ischemia is when there is an abnormal QRS, such as LVH, LBBB, LV aneurysm (old MI with persistent STE) or WPW." There is upsloping ST elevation in III, with reciprocal ST depression in aVL. You do NOT see this in normal variant STE, nor in pericarditis.
Immediate and early percutaneous coronary intervention in very high-risk and high-risk Non-STEMI patients. A CT was completed to rule out dissection, PE, or aneurysm, and this was unremarkable. Clin Cardiol 2022; [link] Labs included: hsTnI 156 ng/L, Hb 12 g/dL, WBC 12x10^9/L, Cr. mg/dL, K 3.5
Post-myocardial infarction (MI) ventricular septal defects are frequently seen in mid-anteroseptal and apical septal segments, whereas apex and the basal inferior segment are prone to aneurysm formation. These being said, the most important thing in this clinical situation is to diagnose OMI, whatever you call it.
It looks like anterior LV aneurysm. In acute STEMI, the T-wave is large, whereas in LV aneurysm , the T-wave is not so large. If greater than or equal to 0.22 , then acute anterior STEMI. correlates with anterior STEMI) Rule 2. correlates with anterior STEMI). correlates with anterior STEMI).
Thus, this is BOTH an anterior and inferior STEMI in the setting of RBBB. How old is this antero-inferior STEMI? Although acute anterior STEMI frequently has narrow QR-waves within one hour of onset (1. the presence of such well developed, wide, anterior Q-wave suggests completed transmural STEMI. Could it be acute (vs.
Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Note that they finally have laid to rest the new or presumably new LBBB as a criteria for STEMI. Also note that they allow ST depression c/w posterior MI to be a STEMI equivalent. What is the utility of a head CT in cardiac arrest?
There is a very small amount of STE in some of the anterior, lateral, and inferior leads which do NOT meet STEMI criteria. The case was reviewed by all parties, and it was stated correctly that the ECG does not meet the STEMI criteria. The STEMI vs. NSTEMI paradigm is not the best way to decide who needs emergent reperfusion therapy.
It may be difficult to read STEMI in the setting of RBBB. There is, however, a long QT also, with abnormal T-waves, but this is not STEMI. An elderly patient with a ruptured abdominal aortic aneurysm: Formal ECG Interpretation (final read in the chart!) : "Inferior ST elevation, lead III, with reciprocal ST depression in aVL."
50% of LAD STEMIs do not have reciprocal findings in inferior leads, and many LAD OMIs instead have STE and/or HATWs in inferior leads instead. The ECG easily meets STEMI criteria in all leads V2-V6, as well. Repeat CT angio chest (not CT coronary, unclear what protocol) showed possible LAD aneurysm and thrombus. Pericarditis?
It is clearly not a STEMI and is therefore a Non-STEMI or NSTEMI.) This shows that the term Non-STEMI is useless, as Non-STEMI can be either OMI or NOMI. This troponin value makes the diagnosis of acute MI almost certain, but this troponin by no means tells you if it is OMI or Non-OMI (NOMI).
Not quite a STEMI, but same effect.) There is ST elevation in V2-V4 that does not quite meet "STEMI criteria." You might think it is "Old MI with persistent ST Elevation" (otherwise known as "LV aneurysm" morphology.") Is this a transient STEMI? When Q-waves have developed, it cannot be assumed to be a transient STEMI.
cm diameter in the apex The presence of thrombus led the clinicians to state that this was a "late presentation STEMI." It does take some time for thrombus to form, but the EKG and the troponin profile show that this was NOT a late presentation STEMI. Perhaps she will not develop an LV aneurysm. LV Thrombus , 1.5
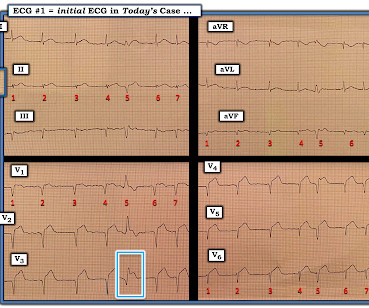
iv ) The findings in Figure-4 could reflect LV aneurysm. This may account for the anterior ST elevation seen in today's case ( BLUE arrows in leads V1,V2,V3 ). C onclusion: As I contemplated today's tracing that I initially interpreted without the benefit of any history I thought any of the above diagnostic possibilities might be present.
Jesse McLaren explains how STEMI criteria can be false positive with large scale QRS and proportional ST elevation, or false negative with low/normal scale QRS and disproportionate ST elevation and hyperacute T waves, and that rules for subtle occlusion using proportionality can help differentiate LBBB with or without Occlusion MI, or LV aneurysm vs (..)
There are no Q-waves to suggest old inferior MI, or inferior aneurysm as the etiology of the ST Elevation. Supply-demand mismatch can cause ST Elevation (Type 2 STEMI). Also see these posts of Type II STEMI. Truly, the Marquette 12 SL algorithm correctly identifies this STEMI. See reference and discussion below.
His initial high sensitivity troponin I returned at 1300 ng/L and given that his cardiac workup was otherwise unremarkable, a CT was obtained to evaluate for pulmonary embolism and aortic aneurysm or dissection but this too was unrevealing. Another EKG was also obtained. ECG at time 82 minutes: What do you think?
It is consistent with an inferior LV aneurysm. Queen : she saw no OMI (no "STEMI Equivalent") either Continued : Now, she says she was walking to the bathroom when she experienced acute onset substernal chest pressure radiating into her neck and left arm. It is almost certainly not acute.
The cath lab was deactivated by cardiologist on arrival at ED because it was "not a STEMI". No thoracic aortic hematoma, aneurysm or dissection. Pt received 324 ASA and 2 sprays of nitro with improvement. Cath lab was activated by EMS and transported emergent." Pain was decreased to 2/10. CT Angio Chest IMPRESSION 1.
We organize all of the trending information in your field so you don't have to. Join thousands of users and stay up to date on the latest articles your peers are reading.
You know about us, now we want to get to know you!
Let's personalize your content
Let's get even more personalized
We recognize your account from another site in our network, please click 'Send Email' below to continue with verifying your account and setting a password.














































Let's personalize your content